Category: Ataxia
Objective: To report the first Indian patient with SCA 40 who presented in the fifth decade with a novel missense mutation (c.1291C>T, p.His431Tyr), expanding the catalog of pathogenic variants in SCA-40.
Background: Spinocerebellar ataxias (SCAs) are hereditary neurodegenerative disorders with over 40 subtypes linked to various gene mutations, usually in an autosomal dominant pattern.[1-2] Among these, Spinocerebellar Ataxia Type 40 (SCA-40) is a rare form linked to mutations in the CCDC88C gene, which encodes a protein involved in neuronal signaling.[3-4] SCA-40 usually presents with gait imbalance, dysarthria, and oculomotor abnormalities. Diagnosing SCA-40 is challenging due to overlapping features with other SCAs. Standard genetic panels may miss rare mutations, making whole exome sequencing (WES) essential.
Method: We report a case of SCA-40 in a 55-year-old Indian female who presented with a two-year history of progressive imbalance, frequent falls, and speech changes. Neurological examination revealed restricted vertical gaze, slow horizontal saccades, cerebellar dysarthria, and impaired coordination with a tendency to sway during walking.
Results: Routine metabolic, autoimmune, and paraneoplastic profiles were normal, and MRI showed cerebellar and midbrain atrophy. The initial SCA panel was negative, prompting whole exome sequencing (WES), which identified a novel missense mutation (c.1291C>T, p.His431Tyr) in the CCDC88C gene. Classified as a Variant of Unknown Significance (VUS), this mutation was reclassified as likely pathogenic based on in-silico analysis and ACMG guidelines. Reverse phenotyping correlated oculomotor abnormalities and cerebellar ataxia with SCA-40 features, though genetic heterogeneity complicates phenotype-genotype correlation. Segregation analysis supported a de novo mutation, as neither her mother nor brother carried the variant, and her father’s sample was unavailable. In this case, the VUS identified via WES required careful reclassification and segregation analysis to support pathogenicity, emphasizing the importance of genetic counselling for understanding novel findings. Treatment for SCA-40 remains supportive, as no disease-specific therapies exist.
Conclusion: This case underscores the role of WES in diagnosing rare ataxias and highlights the need for a multidisciplinary approach combining clinical phenotyping, genetic analysis, and counselling to support individualized care.
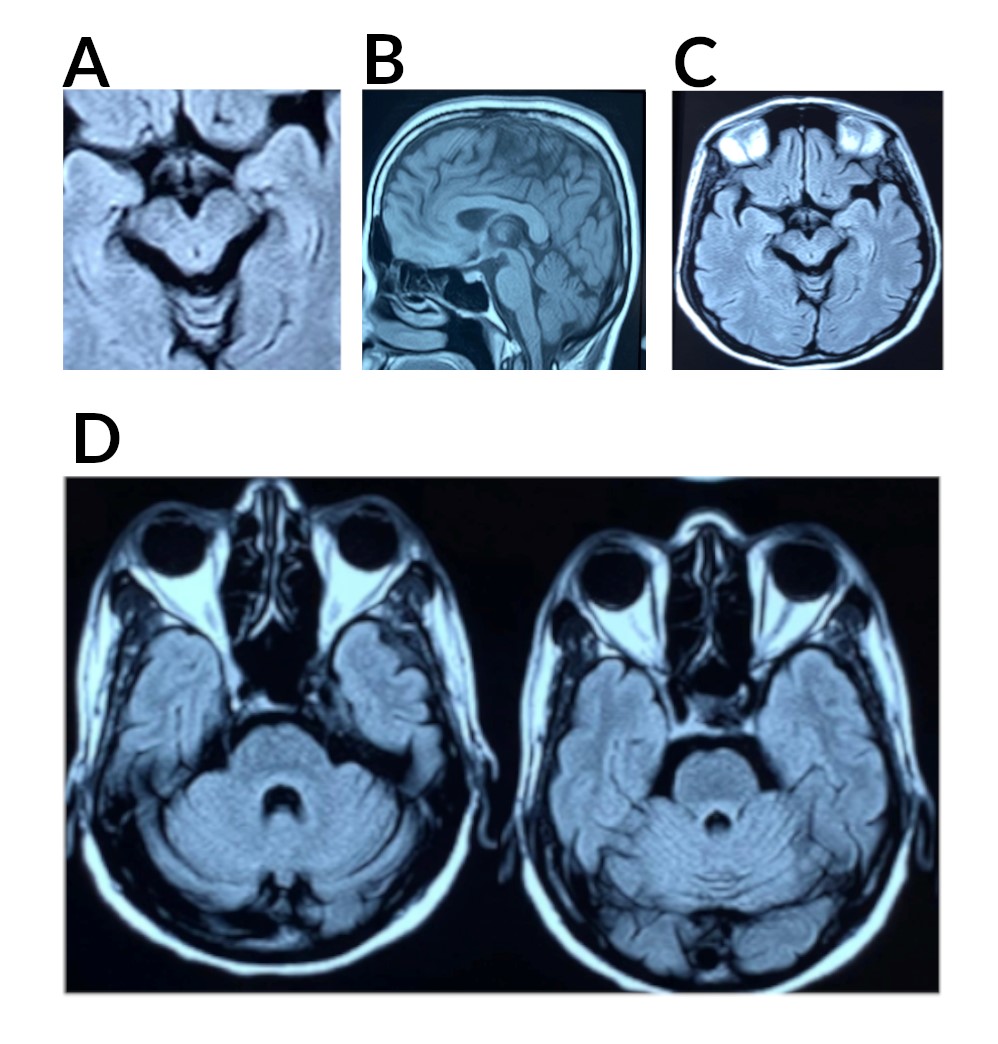
Figure 1: Sagittal and Axial MRI Brain Plain
References: 1. Bhandari J, Thada PK, Samanta D. Spinocerebellar Ataxia. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 [cited 2024 Nov 1]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK557816/
2. Emamikhah M, Aghavali S, Moghadas F, Munhoz RP, Lang AE, Alavi A, et al. Spinocerebellar Ataxia 40: Another Etiology Underlying Essential Tremor Syndrome. Mov Disord Clin Pract. 2021;8:944–946.
3. Boros FA, Szpisjak L, Bozó R, Kelemen E, Zádori D, Salamon A, et al. Spinocerebellar Ataxia in a Hungarian Female Patient with a Novel Variant of Unknown Significance in the CCDC88C Gene. Int J Mol Sci. 2023;24:2617.
4. Chai S, Liu D, Liu Y, Sang M. A Novel c.3636-4 A>G Mutation in the CCDC88C Plays a Causative Role in Familial Spinocerebellar Ataxia. Hum Hered. 2023;88:91–97.
5. Han F, Su D, Qu C. Spinocerebellar ataxia type 40: A case report and literature review. Transl Neurosci. 2021;12:379–384.
To cite this abstract in AMA style:
A. Mehta, P. Hiremath, M. Javali, P. R, L. Priya, P. Acharya. Spinocerebellar Ataxia Type 40 (SCA-40) with a Novel Mutation in an Indian Female: A Case Report [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/spinocerebellar-ataxia-type-40-sca-40-with-a-novel-mutation-in-an-indian-female-a-case-report/. Accessed July 7, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/spinocerebellar-ataxia-type-40-sca-40-with-a-novel-mutation-in-an-indian-female-a-case-report/