Category: Choreas (Non-Huntington's Disease)
Objective: The relationship between movement disorders and renal diseases is complex and multifaceted. Movement disorders can occur as manifestations of azotemia (uremic encephalopathy, uremic striatopallidal syndrome, and restless leg syndrome), manifestations of electrolyte abnormalities arising out of renal dysfunction, consequences of complications arising from dialysis, consequences of complications arising from renal transplantation, and manifestations of drug toxicity in the setting of renal dysfunction.
Background:
Case report
A 62-year-old Dominican man with Diabetes mellitus, arterial hypertension, and chronic renal failure on hemodialysis presented to our movement disorders clinic for evaluation of sudden onset of a hyperkinetic movement disorders characterized by generalized involuntary movements of the head trunk and upper and lower limbs that began 3 days prior. The movements were not suppressible and there was no family history of abnormal movements. (Video 1)
Method: An emergency department evaluation the blood urea nitrogen of 67 mg/dL, and serum creatinine of 9.6 mg/dL; Sodium: 137 mmol/L, Calcium: 8.6 mg/dL, Phosphorus: 3.9 mg/dL, Magnesium: 1.85 mg/dL, Potassium: 5.00 mmol/L, Iron: 61, TIBC: 161, Ferritin: 2374, Intact PTH: 387 (pg/mL). He was medicated with haloperidol at the emergency room, and hospitalization to optimize hemodialysis therapy. A magnetic resonance imaging (MRI) brain was obtained showing basal ganglia hyperintensity in T2W and FLAIR images. (Figure 1).
Results: It is important to highlight in the context of hypertensive crisis 3 years prior, a cranial magnetic resonance imaging had been performed without involvement of the nigrostriatal pathway. (Figure 2.) He was diagnosed with uremic striatopallidal syndrome. Furthermore, in the case of this patient, hyperparathyroidism secondary to kidney disease was taken into account as an aggravating factor. At follow up in our clinic 1 month later, he reported that the movements started to improve after optimized the hemodialysis therapy.
Conclusion: Discussion
The abnormalities of uremic striatopallidal syndrome are characterize of Parkinsonism or chorea depending on predominant involvement of the GPi or GPe respectively. The prognosis in chorea usually improves within days to weeks with intensification of hemodialysis; use of dopamine receptor blockers for chorea may cause parkinsonism; neurological symptoms may persist despite radiological resolution.
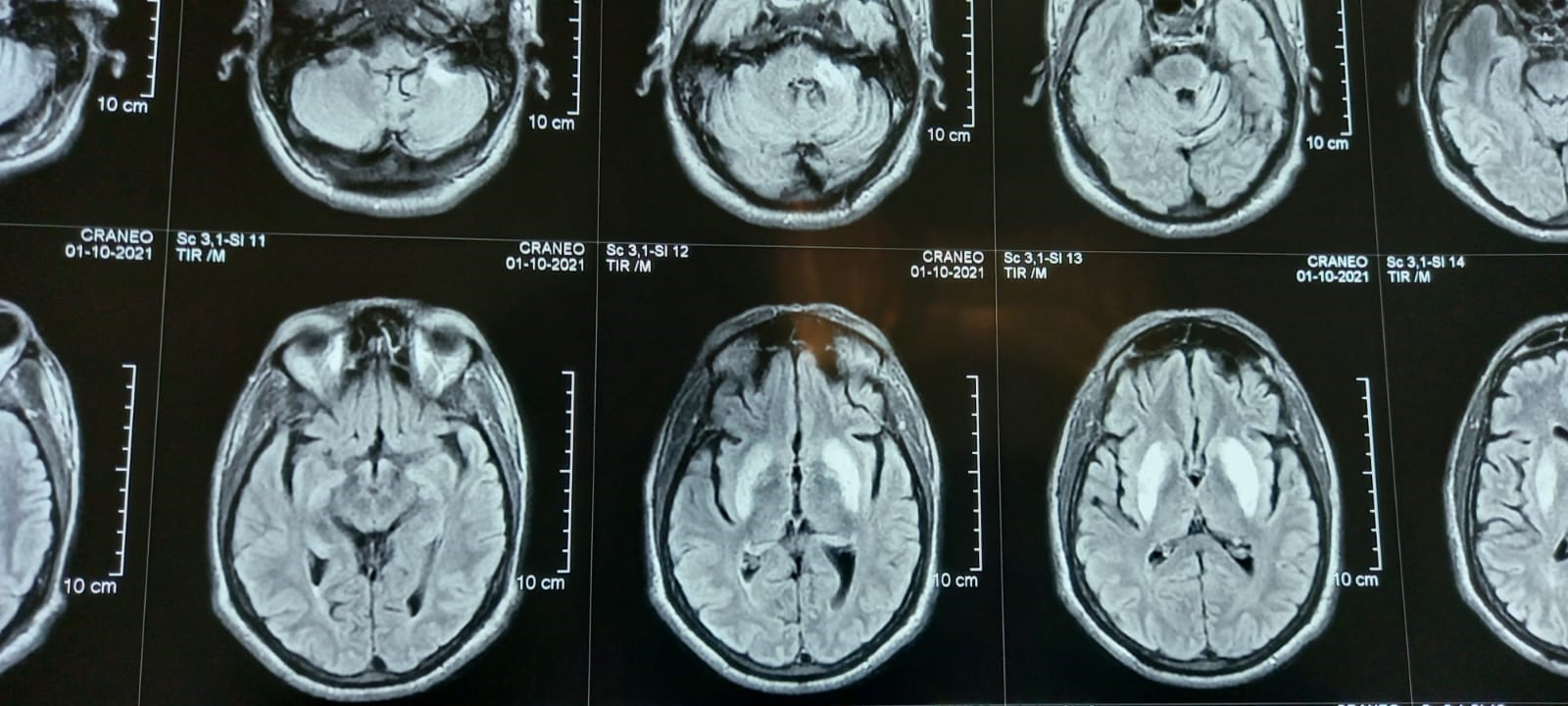
Figure 1. MRI
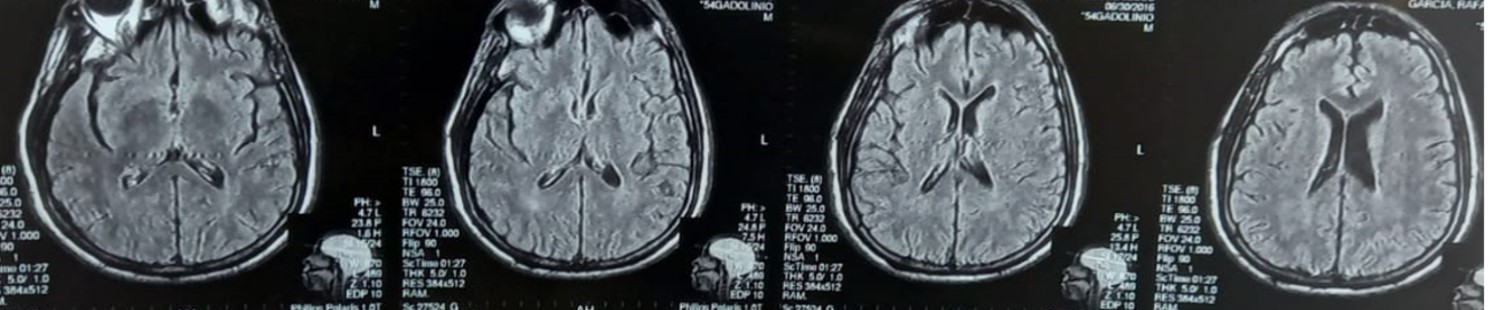
Figure. 2 MRI
References: 1- Bhowmick SS, Lang AE. Movement Disorders and Renal Diseases. Mov Disord Clin Pract. 2020 Aug 10;7(7):763-779. doi: 10.1002/mdc3.13005. PMID: 33043074; PMCID: PMC7534014.
2 – Forbes E, Vaswani PA, Duda JE, Morley JF. Uremic Striatopallidal Syndrome Manifesting as Acute Onset Chorea. Mov Disord Clin Pract. 2021 Sep 3;8(Suppl 1):S55-S57. doi: 10.1002/mdc3.13285. PMID: 34514054; PMCID: PMC8414490.
3- Kim DM, Lee IH, Song CJ. Uremic encephalopathy: MR imaging findings and clinical correlation. Am J Neuroradiol 2016;37(9):1604–1609. [DOI] [PMC free article] [PubMed] [Google Scholar]
To cite this abstract in AMA style:
R. Cruz Vicioso, J. Carbonell, C. Pérez. Uremic Striatopallidal Syndrome Manifesting As Acute Onset Chorea [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/uremic-striatopallidal-syndrome-manifesting-as-acute-onset-chorea/. Accessed July 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/uremic-striatopallidal-syndrome-manifesting-as-acute-onset-chorea/