Category: Choreas (Non-Huntington's Disease)
Objective: To describe three unrelated cases of Chorea-acanthocytosis (ChAc) from Puerto Rico, featuring heterozygous and homozygous pathogenic variants
Background: ChAc, a rare autosomal recessive neurodegenerative disorder, is caused by homozygous or compound heterozygous pathogenic variants in the VPS13A gene, which encodes the chorein protein [1]. Clinical manifestations may involve chorea, orofacial dyskinesia, dysphagia, dysarthria, neuropsychiatric symptoms, seizures, peripheral neuropathy, myopathy, or parkinsonism [2].
Method: Case series
Results: Case A: A 34 year-old female with a history of focal epilepsy was referred with progressive dysphagia, dysarthria, and slight head tremor. On examination, she exhibited a premonitory urge for repetitive, constant, involuntary vocalizations. Additionally, she presented with orobuccolingual chorea and dystonia. Laboratory studies, including creatine phosphokinase (CPK), aldolase, and hepatic enzymes, were within normal levels.
Case B: A 36-year-old male misdiagnosed with Tourette syndrome (TS) was referred with involuntary head movements, left hand postural tremor, gait instability with falls, dysarthria, and dysphagia. On examination, he presents a premonitory urge of vocalizations. Later, he progressed to develop seizures. Laboratory studies revealed elevation of hepatic enzymes and CPK levels. Western blot of erythrocyte membranes demonstrated absence of chorein.
Case C: A 16-year-old male was found to have unexplained elevated hepatic enzymes and CPK levels during a hospitalization for pancreatitis at age 14. He later underwent genetic evaluation, which confirmed ChAc with a homozygous VPS13A pathogenic variant. He sought neurological evaluation but remains asymptomatic for now.
Whole exome sequencing (WES) identified the same pathogenic variant in the VPS13A gene; c.3889C>T (p.A1297T), for both Case A and Case B. Another likely pathogenic variant, c.3961-2A>C, not previously reported, was identified in Case A. WES identified the pathogenic variant: c.3556C>T (p.V1187L) for Case C; a variant previously reported in another Puerto Rican patient [3].
Conclusion: This case series highlights the clinical variability of ChAc in Puerto Rican patients and the role of genetic testing in identifying pathogenic VPS13A variants, advancing our understanding of the disease in this population.
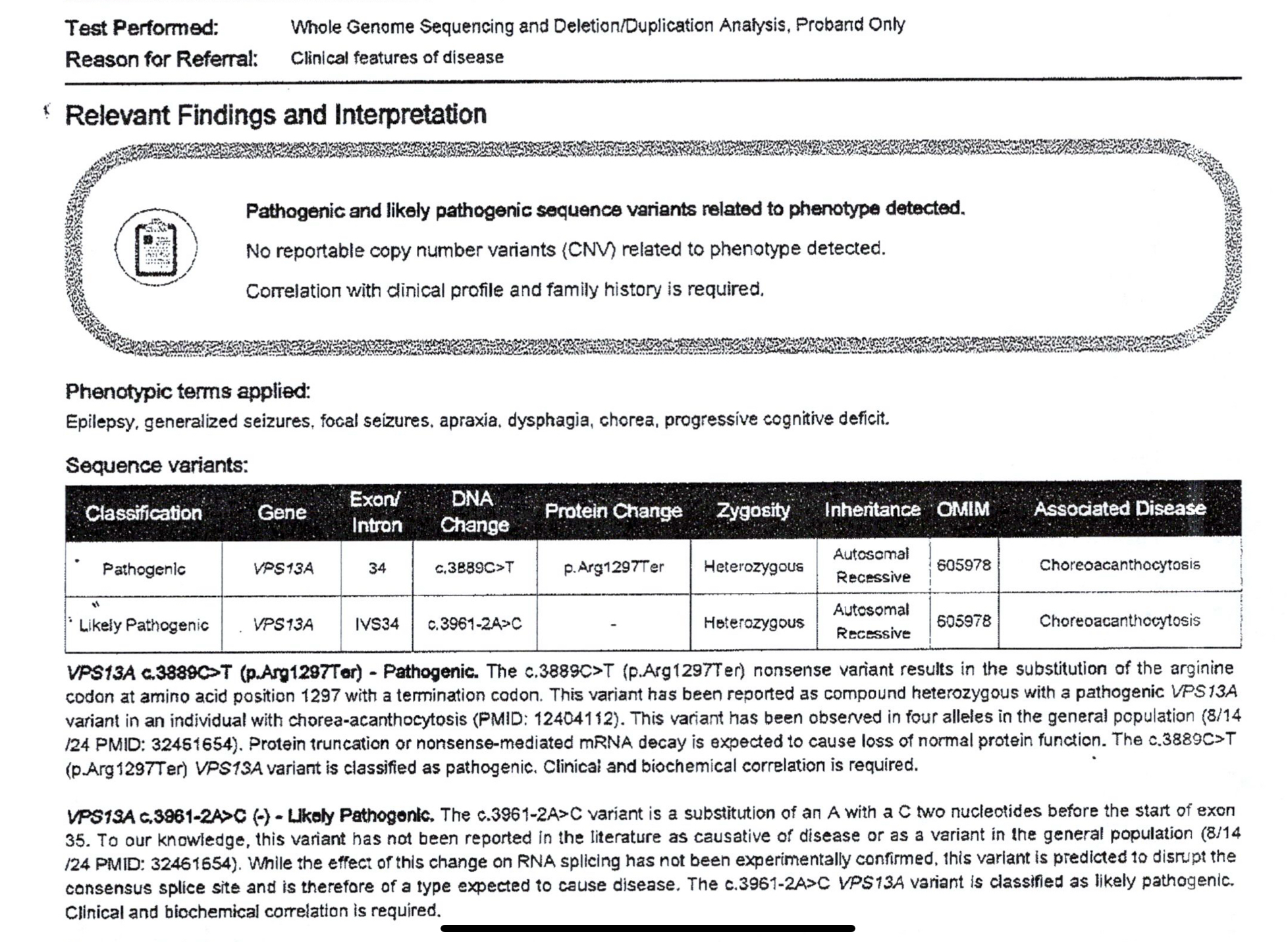
Case A genetic test report
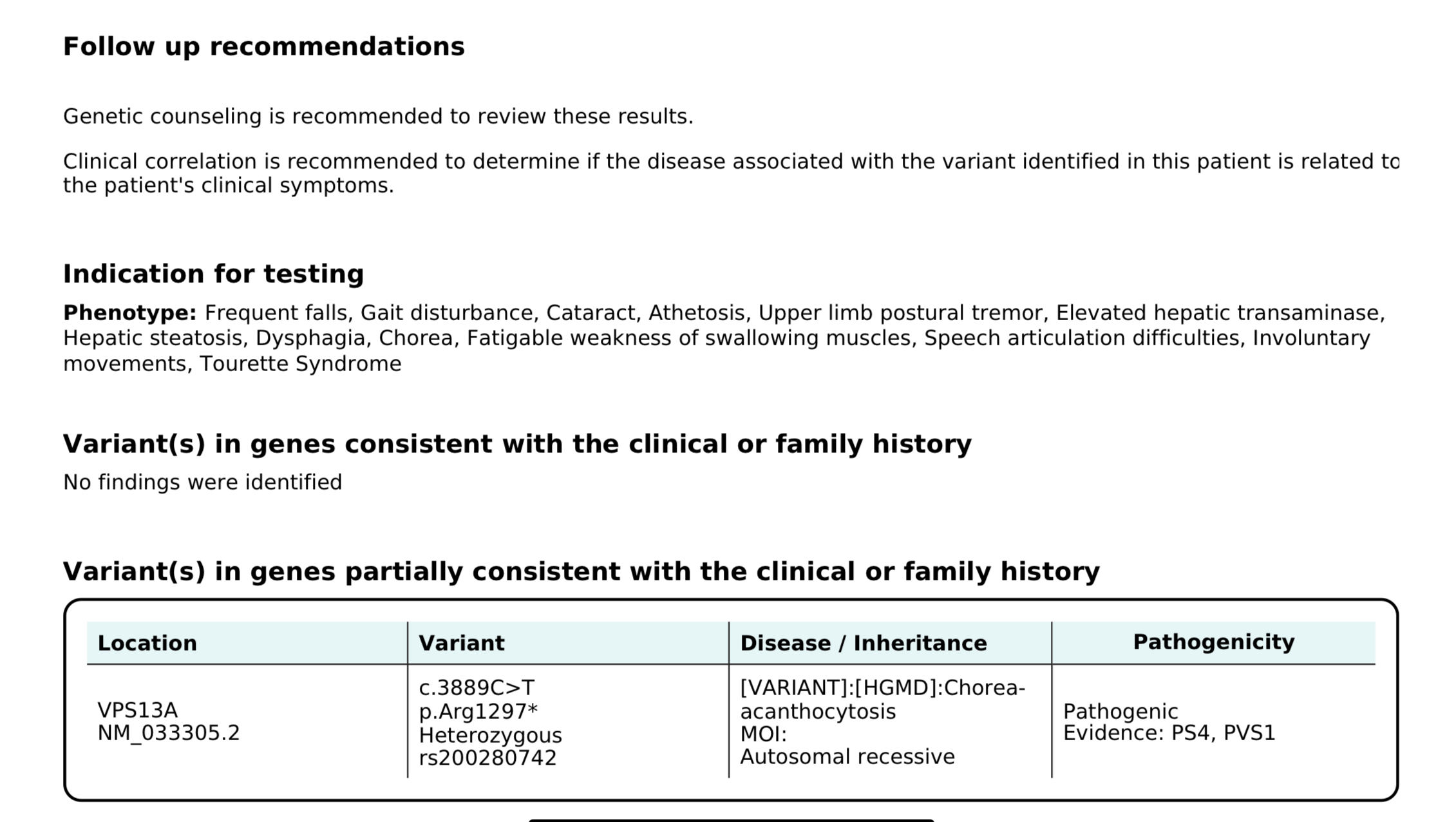
Case B genetic test report
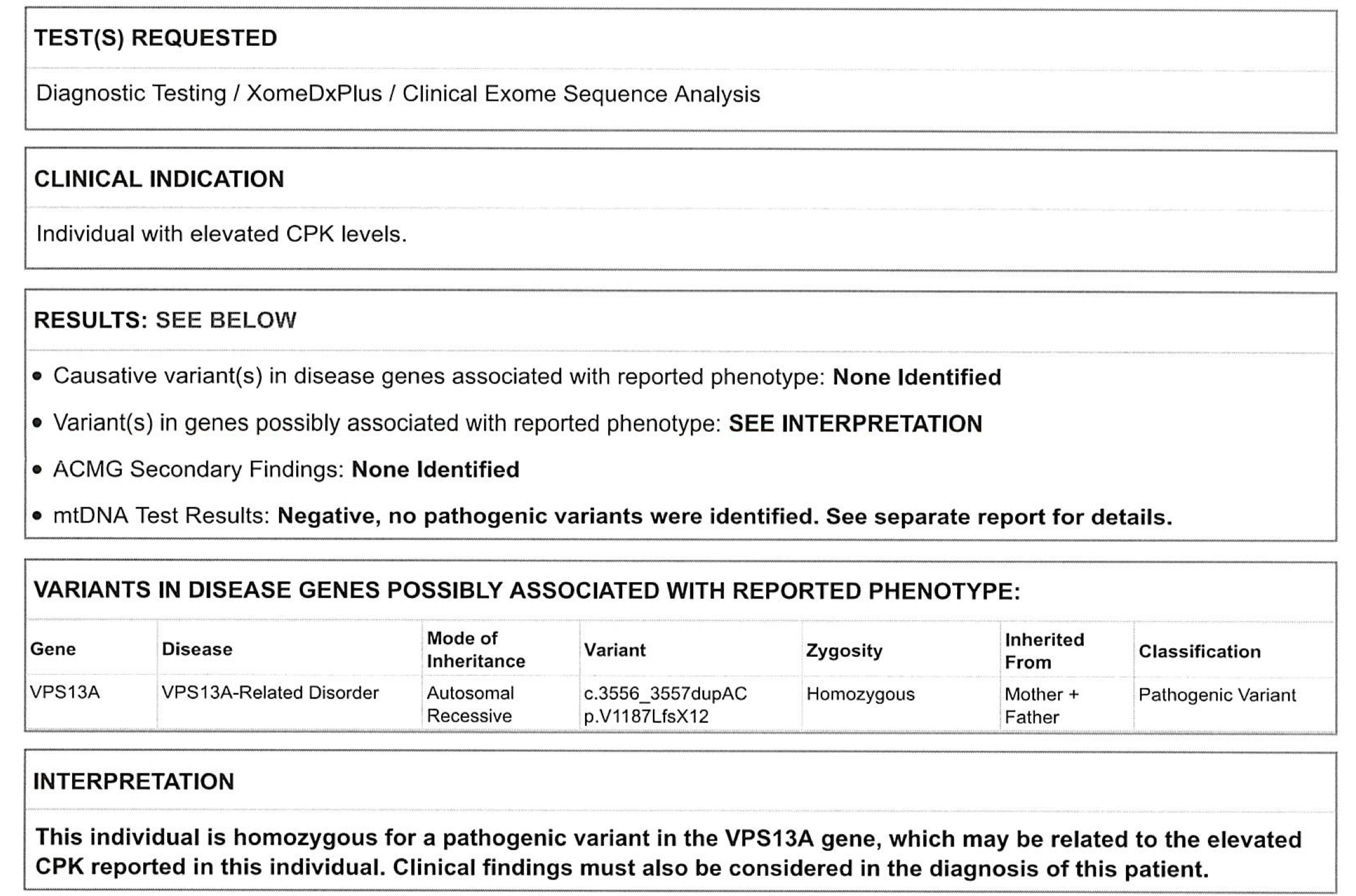
Case C genetic test report
References: [1] Jung HH, Danek A, Walker RH. Neuroacanthocytosis syndromes. Orphanet J Rare Dis. 2011;6:68. Published 2011 Oct 25. doi:10.1186/1750-1172-6-68
[2] Lang F, Pelzl L, Schöls L, et al. Neurons, Erythrocytes and Beyond -The Diverse Functions of Chorein. Neurosignals. 2017;25(1):117-126. doi:10.1159/000485457
[3] Walker RH, Schulz VP, Tikhonova IR, et al. Genetic diagnosis of neuroacanthocytosis disorders using exome sequencing. Mov Disord. 2012;27(4):539-543. doi:10.1002/mds.24020
To cite this abstract in AMA style:
E. Pérez-Luciano, C. Chapel-Crespo, D. Lozada-Figueroa, I. Pita-García, L. Surillo-Dahdah. Chorea-acanthocytosis in Puerto Rico: A Case Series [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/chorea-acanthocytosis-in-puerto-rico-a-case-series/. Accessed July 8, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/chorea-acanthocytosis-in-puerto-rico-a-case-series/