Category: Dystonia: Genetics
Objective: To describe phenotypic variability associated with a GCH1 mutation and increase clinical suspicion in patients with atypical phenotypes.
Background: Dopa-responsive dystonia (DRD) is a genetic disorder most commonly caused by mutations in the GCH1 gene, which affects catecholamine metabolic pathways notably responsible for dopamine production. Clinically, DRD often presents as childhood or adolescent-onset fluctuating limb dystonia that improves dramatically with levodopa. However, the phenotype can vary, leading to misdiagnosis and delayed treatment.
Method: We report a family with varying symptoms due to a single GCH1 mutation where one of the initial diagnoses was multiple sclerosis (MS).
Results: A 73-year-old woman was referred to the movement disorder clinic for progressive walking difficulty with stiffness in her right leg. She had been initially investigated at age 46 by a general neurologist. A brain MRI had reveled bilateral frontoparietal and periventricular white matter lesions compatible with MS, and a repeat MRI showed progression of her white mater lesions. The patient was diagnosed with primary progressive MS.
Several years after her diagnosis, her 40-year-old son was referred to our clinic and was diagnosed with young-onset Parkinson’s disease. His DAT scan was positive for nigrostrial degeneration and a genetic panel showed a CGH1 mutation (c.164T>A).
Upon her son‘s genetic diagnosis, the patient was referred to our clinic. Her symptoms, initially considered asspasticity, were attributed to leg dystonia, and markedly improved upon initiation of dopaminergic agents. Genetic panel confirmed the same mutation CGH1 mutation.
Two other family members subsequently consulted for long-standing symptoms of parkinsonism, one of whom alsopresented with unilateral lower limb dystonia.
Conclusion: To the best of our knowledge, this is the first case of DYT5 masquerading as MS. MS-like white matter changes on the MRI can be a misleading feature, complicating the diagnosis. Early recognition of DRD, especially in families with a history of neurological symptoms, is essential for initiating effective treatment with levodopa and preventing unnecessary interventions. This series demonstrates how DRD can mimic MS, emphasizing the need for heightened clinical awareness and the role of genetic testing in making an accurate diagnosis.
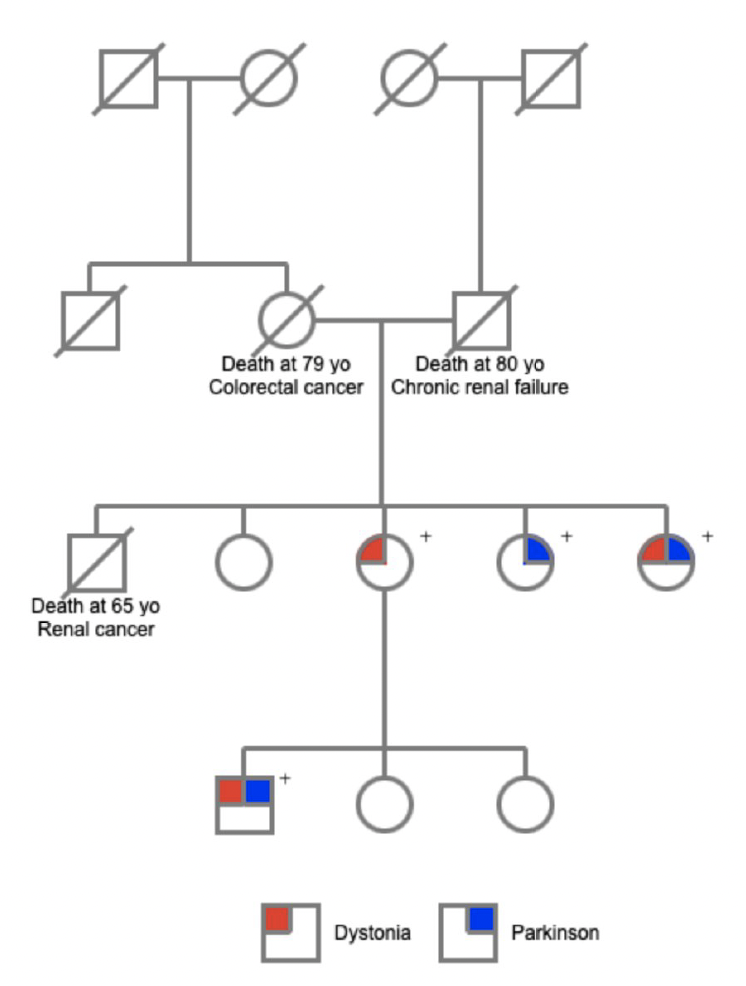
Figure 1 – genealogic tree
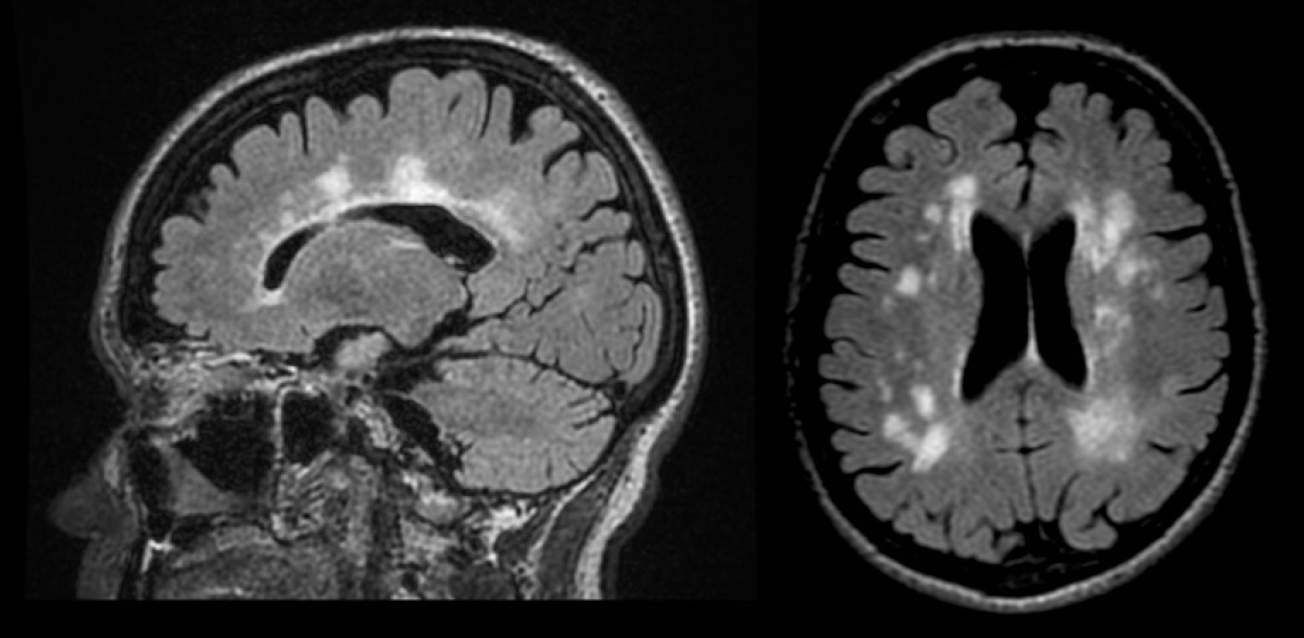
Figure 2 – MRI
To cite this abstract in AMA style:
B. Perraud, I. Beaulieu-Boire. When Dystonia mimics Multiple Sclerosis : A Familial case series of GCH1 misdiagnosis [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/when-dystonia-mimics-multiple-sclerosis-a-familial-case-series-of-gch1-misdiagnosis/. Accessed July 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/when-dystonia-mimics-multiple-sclerosis-a-familial-case-series-of-gch1-misdiagnosis/