Category: Dystonia (Other)
Objective: To study the clinical course, imaging, diagnosis and management of a case of acute onset of left laterocollis with jerky dystonic tremor with suspected of hyperglycemia related dystonia in known case of Type 1 Diabetes Mellitus (T1DM).
Background: Hyperglycemia-Induced Involuntary Movements (HIIM) include Hemichorea-Hemiballismus (HCHB), hand tremors but dystonia is rare.1 There is often presentation of hyperintensity involving basal ganglia on MR T1 weighted image2. Neurologic damage in HIIM may be explained by GABA depletion, vascular insufficiency or hyperosmolar insult.3
Method: A 32 year old, insulin dependent diabetic male from West India presented with acute onset of left laterocollis with jerky dystonic tremor for 2 days. There was neither any history of loss of consciousness, focal neurological deficits or other abnormal movement, nor any neuroleptic or anti-emetic drug exposure. He had severe rheumatic mitral stenosis and Tricuspid regurgitation for which, mitral valve replacement and tricuspid valve repair was done 2 years ago. He was kept on oral anticoagulant, with history of default of all medications for last 1 week.
On physical examination, he was conscious, oriented and following commands. All cranial nerve, motor examination, cerebellar examination and sensory examination was normal. He has left laterocollis with jerky dystonic tremor.
Results: On admission, his blood glucose was 420mg/dl, HbA1c was 12.2% (Normal <6%), serum osmolality of 279mOsm/Lit (Normal 275-295), and INR of 1.35. Electrolytes, Renal function and Liver function test was normal. EEG was normal. MRI Brain shows chronic microbleeds in bilateral cerebral and cerebellar hemisphere (Fig-1). The dystonic tremors and neck dystonia were completely controlled after achieving target range glycemic control with insulin, and was discharged on insulin and oral anticoagulant treatment.
Conclusion: HIIM could be due to HCHB or tremor, often associated with signal changes in basal ganglia on MRI. Focal dystonia, as described here, is not as commonly reported (only 2 cases reported till the date) and highlights the occurrence of other movement disorders associated with hyperglycemia with possibly normal imaging. Understanding the complex presentation of patients with HIIM is pivotal for effective patient diagnosis and treatment.
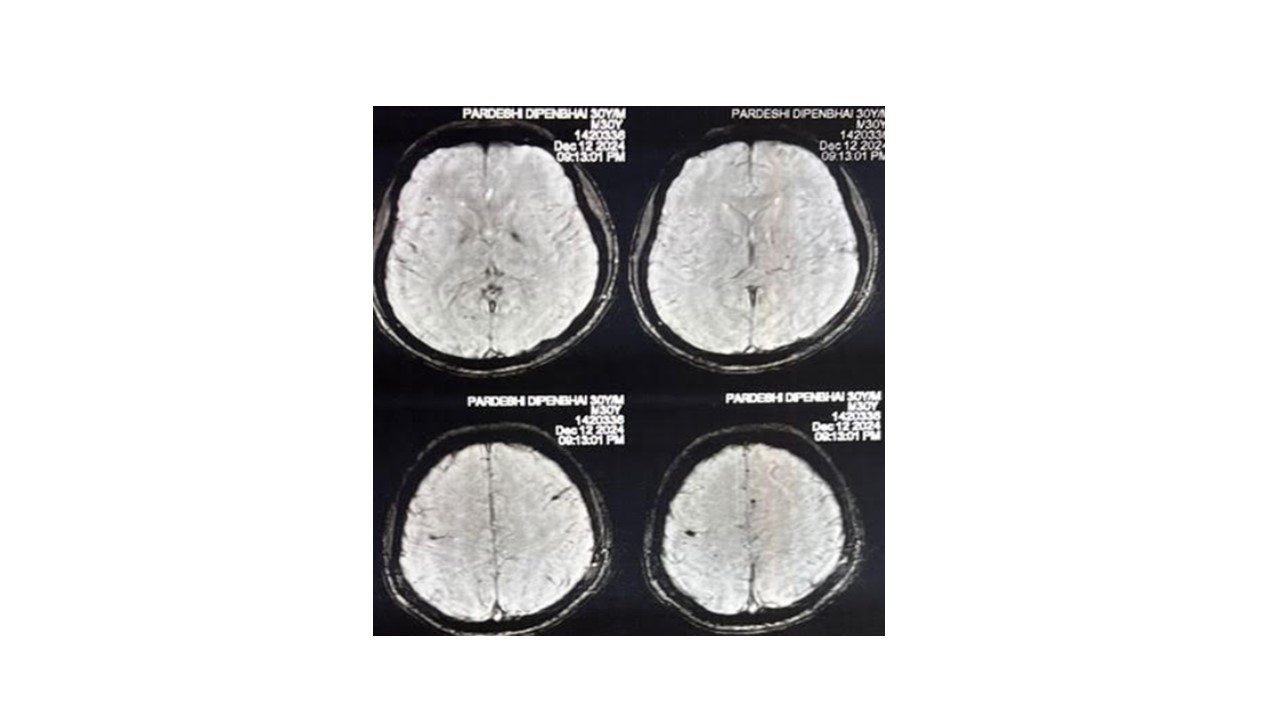
SWI-chronic microbleeds in B/L cerebral hemisphere
References: 1. Humphries N, Gogia B. Acute Focal Dystonia as a Presentation of Uncontrolled Hyperglycemia. Cureus. 2024 Oct 10;16(10).
2. D’Angelo R, Rinaldi R, Pinardi F, Guarino M: Acute chorea-dystonia heralding diabetes mellitus . BMJ Case Rep. 2013, 2013:bcr2013009221.
3. Luna R, Talanki Manjunatha R, Bollu B, et al.: A comprehensive review of neuronal changes in diabetics . Cureus. 2021, 13:e19142.
To cite this abstract in AMA style:
H. Chovatiya. Acute onset of left laterocollis with jerky dystonic tremor as a presentation of uncontrolled hyperglycemia [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/acute-onset-of-left-laterocollis-with-jerky-dystonic-tremor-as-a-presentation-of-uncontrolled-hyperglycemia/. Accessed July 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/acute-onset-of-left-laterocollis-with-jerky-dystonic-tremor-as-a-presentation-of-uncontrolled-hyperglycemia/