Objective: To compare the effect of body position on CNS and PNS function and associated adductor-type laryngeal dystonia (AdLD) voice symptomatology.
Background: Body position impacts voice quality and vocal effort in normal and voice disordered speakers [1-4]; altered head and body posture also influence brain function and laryngeal muscle activation patterns. [5-7] The pathophysiology of AdLD has been investigated using fMRI which requires supine posturing during speaking tasks [8-13]. The comparability of AdLD CNS, PNS, and speech patterns in upright vs supine position is unstudied and would inform changes in brain and neuromuscular function predicted by body position vs disease-specific abnormalities.
Method: A pilot study of voice acoustic measures, laryngeal electromyography (LEMG), and functional near-infrared spectroscopy (fNIRS) was conducted in supine vs upright position during connected speech tasks; acoustic measures were compared in 14 participants, LEMG in 4/14, and fNIRS in 1/14 participants.
Results: Differences associated with body position were evidenced for voice quality with smoothed cepstral peak prominence (CPPs); [14-15] CPPs improved for 13/14 participants in supine vs upright, 7/14 significantly (p<.001; Cohen’s d=.75) [figure1]. Bilateral LEMG measures exhibited variability across participants [figure2]; despite this, moderate to large effect sizes in upright vs supine were shown for decreased amplitude/increased latency of right thyroarytenoid (TA) (d=0.61-1.9), and small to large effect sizes for decreased amplitude and latency of the right cricothyroid (CT) (d=.21-1.7). fNIRS showed increased activation in supine vs upright in the supplementary motor area (d=2.1) and inferior parietal cortex (d=1.75), and decreased activation in the prefrontal cortex (d=0.33), left middle frontal gyrus (d=0.96), right middle frontal gyrus (d=0.61), and postcentral gyrus (d=0.32) [figure3].
Conclusion: The evidence from this pilot study suggests that body position changes in those with AdLD may be associated with measurable changes in voice quality and fNIRS activation. There was heterogeneity in LEMG findings between positions; however, medium to large effect sizes were found in the right TA and CT, indicating that possible right-sided predominance in AdLD should be studied further.
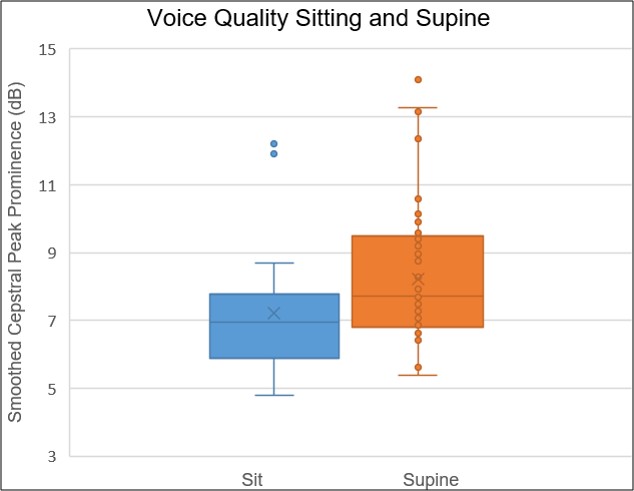
Voice quality improved in supine vs sitting
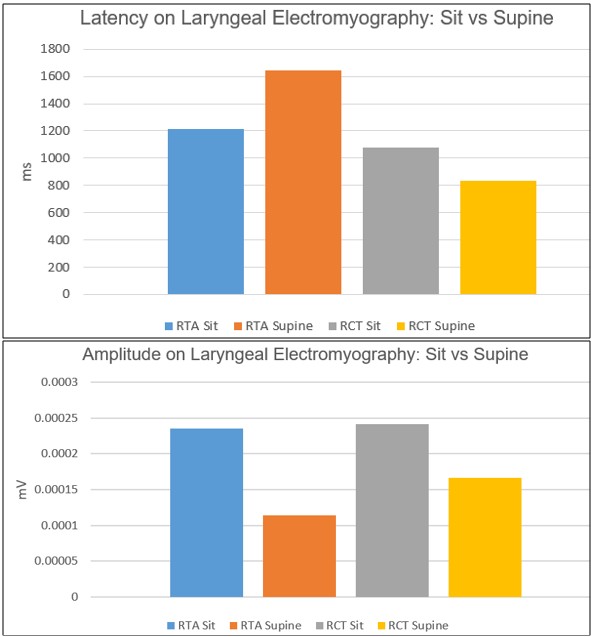
EMG latency and amplitude in right TA and CT
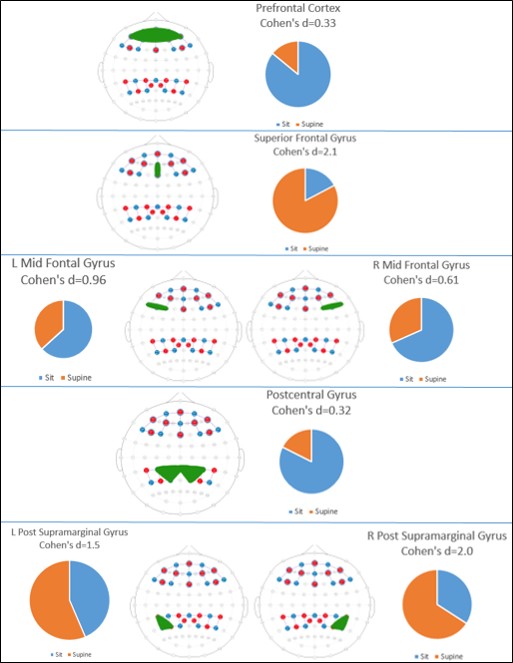
fNIRS results sitting (blue) vs supine (orange)
References: 1. Cardoso R, Lumini-Oliveira J, Meneses RF. Associations between Posture, Voice, and Dysphonia: A Systematic Review. J Voice. 2019;33(1):124 e121-124 e112.
2. Mautner HD. An acoustic and electroglottographic study of the aging voice with and without an open jaw posture. J Voice. 2015; 29(4): 518 e1-11
3. Gilman M, Johns MM. The effect of head position and/or stance on the self-perception of phonatory effort. J Voice. 2017; 31(1): 131 e1-131 e4
4. Lagier A, Vaugoyeau M, Ghio A, et al. Coordination between posture and phonation in vocal effort behavior. Folia Phoniatr Logop. 2010; 62(4): 195-202
5. Rubin JS, Lieberman J, Harris TM. Laryngeal manipulation. Otolaryngol Clin North Am. 2000; 33(5): 1017-1034
6. Huo C, Zhang M, Bu L, et al. Effective Connectivity in Response to Posture Changes in Elderly Subjects as Assessed Using Functional Near-Infrared Spectroscopy. Front Hum Neurosci. 2018;12:98
7. Wang B, Zhang M, Bu L, Xu L, Wang W, Li Z. Posture-related changes in brain functional connectivity as assessed by wavelet phase coherence of NIRS signals in elderly subjects. Behav Brain Res. 2016;312:238-245
8. Simonyan K, Barkmeier-Kraemer J, Blitzer A, et al. Laryngeal Dystonia: Multidisciplinary Update on Terminology, Pathophysiology, and Research Priorities. Neurology. 2021;96(21):989-1001.
9. Simonyan K. Neuroimaging applications in dystonia. Int Rev Neurobiol. 2018; 143: 1-30
10. Simonyan K, Ludlow CL. Abnormal structure-function relationship in spasmodic dysphonia. Cereb Cortex. 2012; 22(2): 417-425
11. Haslinger B, Erhard P, Dresel C, Castrop F, Roettinger M, Ceballos-Baumann AO. “Silent event-related” fMRI reveals reduced sensorimotor activation in laryngeal dystonia. Neurology. 2005;65(10):1562-1569.
12. Simonyan K, Frucht SJ, Blitzer A, Sichani AH, Rumbach AF. A novel therapeutic agent, sodium oxybate, improves dystonic symptoms via reduced network-wide activity. Sci Rep. 2018;8(1):16111.
13. Battistella G, Fuertinger S, Fleysher L, Ozelius LJ, Simonyan K. Cortical sensorimotor alterations classify clinical phenotype and putative genotype of spasmodic dysphonia. Eur J Neurol. 2016;23(10):1517-1527
14. Marks K, Pierce J, Dwenger K, Barkmeier-Kraemer J. Updates in the assessment and treatment characterization in those with laryngeal dystonia & vocal tremor. One-hour oral seminar. ASHA Convention. Boston, MA. November, 2023
15. Pierce JL, Dwenger K, Jennings S, Sharma A, Smith ME, Barkmeier-Kramer J. Acoustic Measures Most Predictive of Botox Treatment Outcomes in Adductor-type Laryngeal Dystonia. Fall Voice Conference. Podium Presentation. Washington, DC. October, 2023
To cite this abstract in AMA style:
J. Pierce, R. Gillam, B. Kirwan, A. Dorval, A. Hancock, A. Stark, D. Legler, H. da Silva, M. Smith, K. Simonyan, J. Barkmeier-Kraemer. The Effect of Body Position on Cortical and Peripheral Neurophysiology of Adductor-type Laryngeal Dystonia: A Pilot Study [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/the-effect-of-body-position-on-cortical-and-peripheral-neurophysiology-of-adductor-type-laryngeal-dystonia-a-pilot-study/. Accessed July 5, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/the-effect-of-body-position-on-cortical-and-peripheral-neurophysiology-of-adductor-type-laryngeal-dystonia-a-pilot-study/