Objective: To investigate the structural and functional connectivity of patients who respond early after deep brain stimulation (DBS) for dystonia.
Background: DBS is an effective treatment for dystonia, though it often takes weeks or months for significant improvement to be noticeable [1]. However, some patients experience earlier improvements without a clear pattern with respect to symptom distribution and etiology [2]. It is currently unclear whether an early response to DBS is linked to the stimulation of specific fiber tracts or the engagement of a particular brain network.
Method: We conducted a retrospective study of patients with different forms of dystonia who were treated with DBS at the globus pallidus internus (GPi). We defined early responders as having more than 25% improvement of their United Dystonia Rating Scale (UDRS) score in 3 months or less after surgery and typical responders as anyone who experienced 25% improvement in UDRS any time after DBS. We reconstructed the DBS electrodes for each patient and then normalized it to MNI space. We calculated the electrical field magnitude at each voxel, and a model of volume of activated tissue (VAT) by creating a mask of voxels with an e-field magnitude of 0.2 V/m. We performed fiber tracking, and functional network mapping [3].
Results: 46 patients with bilateral GPi-DBS were analyzed. In our cohort, 50% had generalized dystonia, 35% segmental dystonia, and 15% cervical dystonia. Twenty-three patients (50%) were early responders. Compared to typical responders, there was no significant difference in their age of symptom onset, age at surgery, pre-operative UDRS, or post-operative UDRS. There was a significantly higher normalized count of fiber tracts connecting the early responders VAT to the cerebellar cortex lobule IX (p = 0.011), crus I (p = 0.007), and crus II (p = 0.03). There was no significant difference in connectivity to somatomotor cortices. Early DBS response was associated with higher functional connectivity from the VAT to the cerebellar cortex crus I (R = 0.254), crus (R = 0.217), and lobule IX (R = 0.257) [[figure1]].
Conclusion: Early responders have significantly higher structural and functional connectivity to the cerebellar cortex compared to late improvers, while having similar somatomotor cortex connectivity. This could be an effect of cerebellar stimulation on its own, or an additional effect to engaging the cerebellar cortex along the somatomotor areas.
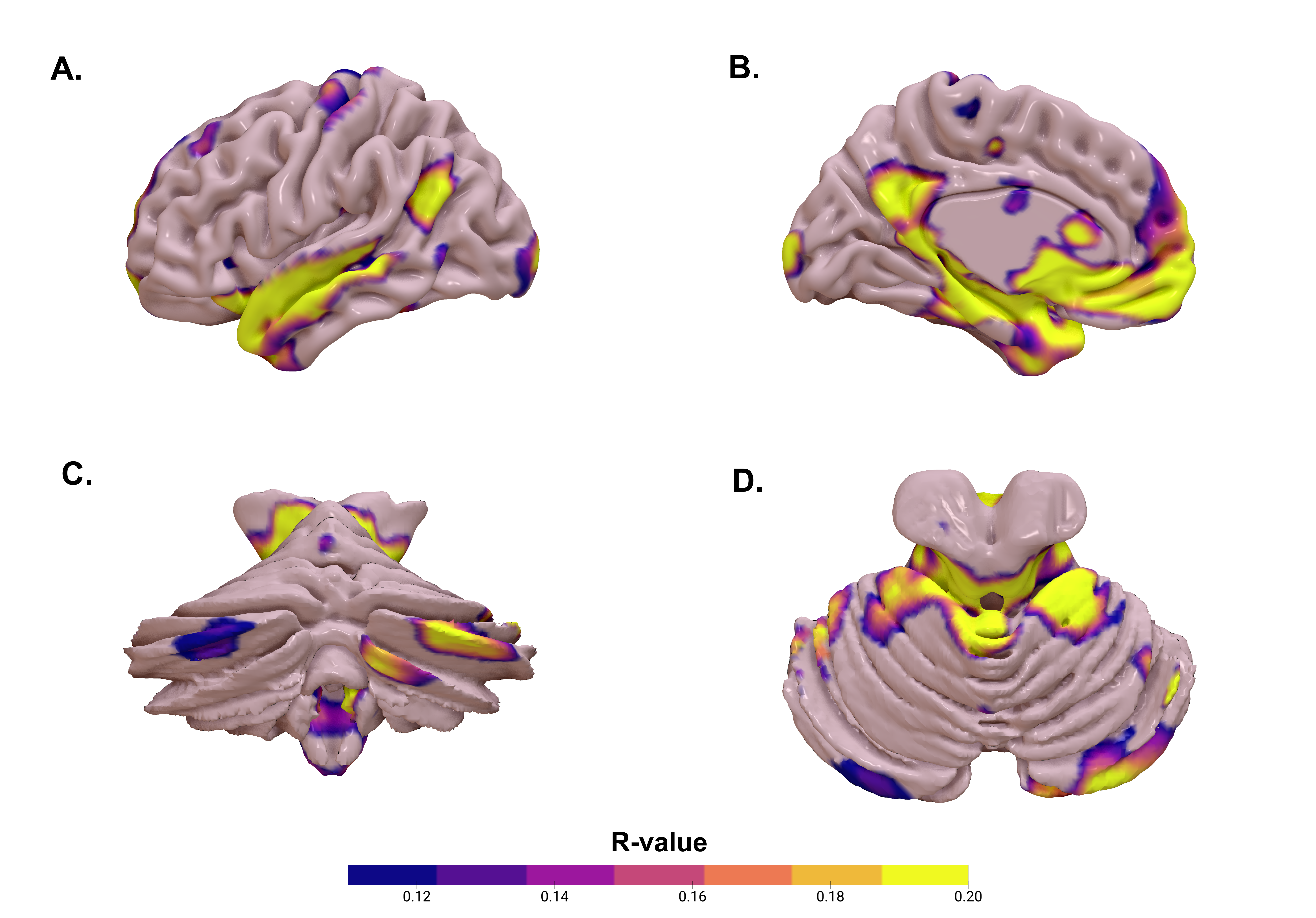
Figure 1
References: 1. Krauss JK, Yianni J, Loher TJ, Aziz TZ. Deep Brain Stimulation for Dystonia: Journal of Clinical Neurophysiology. 2004 Jan;21(1):18–30.
2. Ruge D, Tisch S, Hariz MI, Zrinzo L, Bhatia KP, Quinn NP, et al. Deep brain stimulation effects in dystonia: Time course of electrophysiological changes in early treatment. Movement Disorders. 2011 Aug 15;26(10):1913–21.
3. Horn A, Reich MM, Ewert S, Li N, Al-Fatly B, Lange F, et al. Optimal deep brain stimulation sites and networks for cervical vs. generalized dystonia. Proc Natl Acad Sci USA. 2022 Apr 5;119(14):e2114985119.
To cite this abstract in AMA style:
A. Martinez Nunez, V. Chandra, C. Fleeting, A. Patel, A. Fusco, J. Wong. Cerebellar connectivity predicts early response to GPi-DBS in dystonia. [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/cerebellar-connectivity-predicts-early-response-to-gpi-dbs-in-dystonia/. Accessed July 7, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/cerebellar-connectivity-predicts-early-response-to-gpi-dbs-in-dystonia/