Objective: To determine the risk of worsening or unmasking dystonia following a unilateral High Intensity Focused Ultrasound ventral intermediate thalamotomy (Vim-HiFUS) in medication refractory Essential and Dystonic Tremor (ET/DT).
Background: Thalamic neurosurgical interventions have been reported to worsen or unmask dystonia in tremor-dominant syndromes, an observation we have also made following Vim-HiFUS.1–4 The phenomenon has the potential to change the pattern of motor disability to dystonia in an otherwise successful tremor treatment.
Method: Retrospective blinded video-based analysis of ET and DT patients who underwent a unilateral Vim-HiFUS between November 2018 – April 2022, and returned for research assessments at 1-3 months (short-term) and ≥ 12months (long-term) after treatment, as a part of the prospective study ‘Capturing outcomes in MRgFUS intervention for tremor.’ The primary outcome was the change in total Burke-Fahn-Marsden Rating Scale (BFMRS) after treatment within tremor syndromes. Friedman test was used for within group repeated measures; threshold for statistical significance was considered at a p<0.05. All statistical analysis were conducted using IBM SPSS Statistics (version 29.0.0.0).
Results: Among the 119 patients treated with a unilateral HiFUS ablation between the time interval, 30 patients (15 ET and 15 DT) met the inclusion criteria. The mean cohort age was 72.3 yrs (±9.9) with a median disease duration before treatment of 27.5 yrs (12.5 – 40.0) (Table 1). As expected, DT patients had a greater total BFMRS than ET patients at baseline (DT: 6.0 (3.5 – 7.5); ET: 3.5 (3.0 – 5.0), p=0.029). Though this was not reflected by dystonia in the treated limb (DT: 2.0 (1.0 – 2.0); ET: 2.0 (1.0 – 2.0), p=0.325). The total BFMRS did not significantly change at the short or long-term follow-up in either ET or DT cohorts. In the DT patients, the total BFMRS upper interquartile range (IQR) increased from 7.5 to 9.0 at the long-term follow-up, suggesting a small shift towards higher total BFMRS in this cohort (Table 2).
Conclusion: Unilateral Vim-HiFUS was not associated with a significant increase in BFMRS in the short or long-term. The phenomenon of worsening/unmasking of dystonia after thalamic intervention should be considered rare, at a case report level.
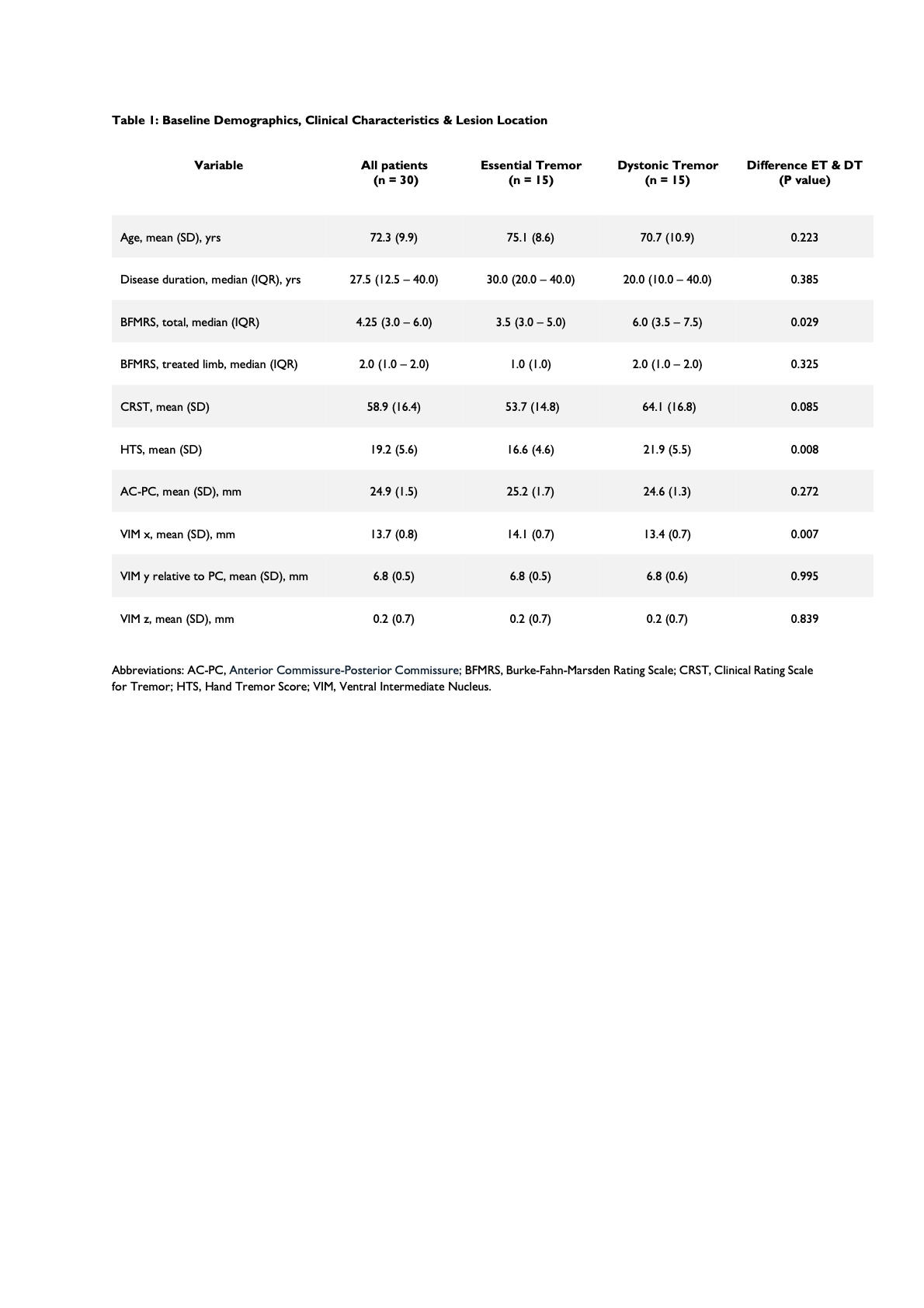
Baseline Demographics
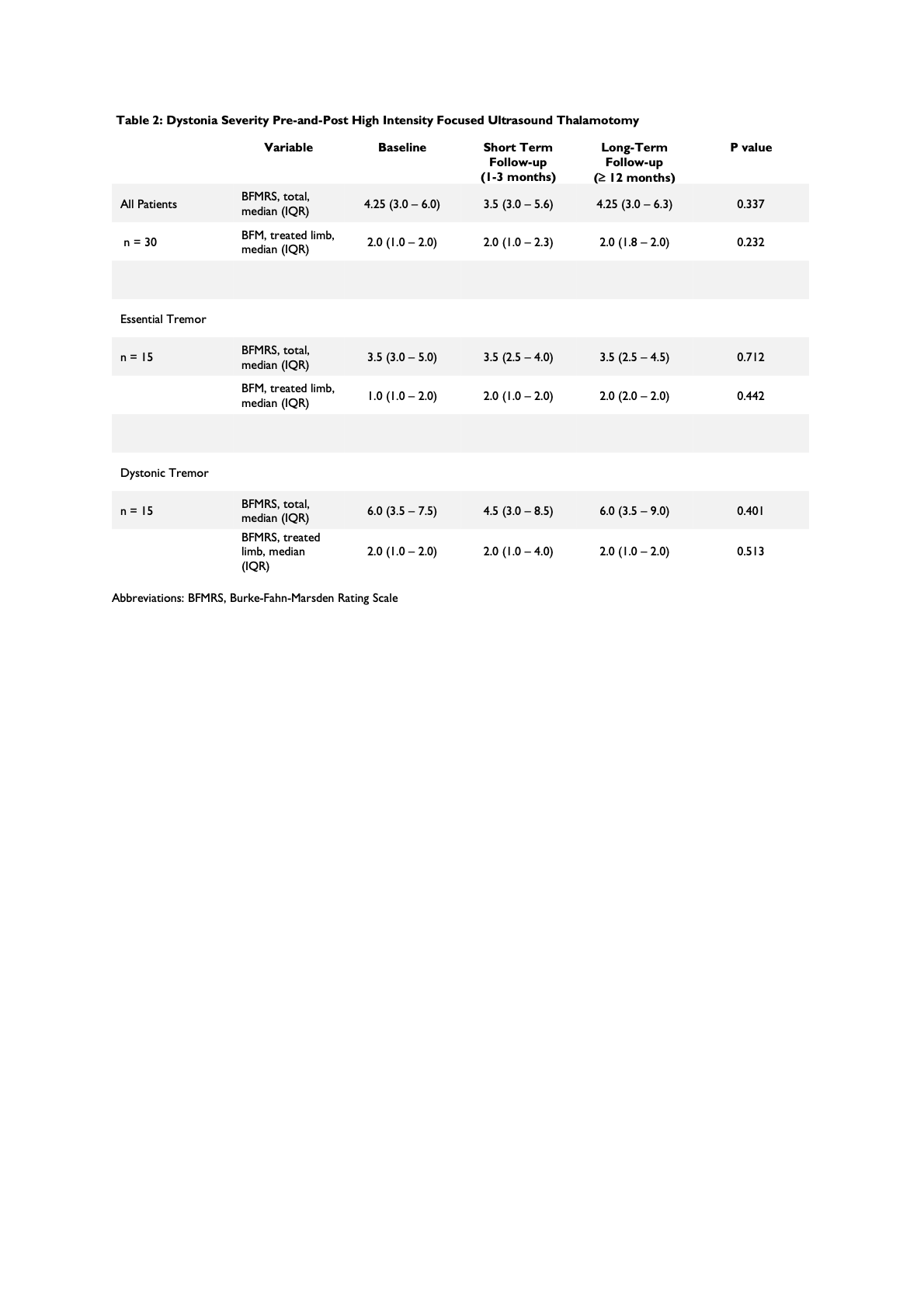
Dystonia Severity Pre-and-Post HiFUS
References: 1. Lee MS, Marsden CD. Movement disorders following lesions of the thalamus or subthalamic region. Mov Disord. 1994;9:493–507.
2. Picillo M, Paramanandam V, Morgante F, et al. Dystonia as complication of thalamic neurosurgery. Parkinsonism & Related Disorders. 2019;66:232–236.
3. Martino D, Rockel CP, Bruno V, et al. Dystonia following thalamic neurosurgery: A single centre experience with MR-guided focused ultrasound thalamotomy. Parkinsonism & Related Disorders. 2020;71:1–3.
4. Peters J, Maamary J, Kyle K, et al. Outcomes of Focused Ultrasound Thalamotomy in Tremor Syndromes. Movement Disorders. Epub 2023 Nov 14.:mds.29658.
To cite this abstract in AMA style:
J. Peters, J. Maamary, K. Kyle, I. Osborne, Y. Barnett, B. Jonker, S. Tisch. Blinded video-based analysis of dystonia before and after unilateral High Intensity Focused Ultrasound thalamotomy in Essential and Dystonic Tremor [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/blinded-video-based-analysis-of-dystonia-before-and-after-unilateral-high-intensity-focused-ultrasound-thalamotomy-in-essential-and-dystonic-tremor/. Accessed July 7, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/blinded-video-based-analysis-of-dystonia-before-and-after-unilateral-high-intensity-focused-ultrasound-thalamotomy-in-essential-and-dystonic-tremor/