Objective: To assess the feasibility of comparing the King’s Pain Disease Pain Scale (KING) and The Parkinson’s Disease Pain Classification System (PD-PCS) in patients with PD, identifying which scale is most suitable for clinical practice in diagnosing and monitoring pain related to PD.
Background: Pain is one of the most common non-motor symptoms (NMS) in PD, with approximately 80% of patients experiencing some form of pain throughout the progression of the disease. Therefore, proper diagnosis and management of this condition are essential to provide comfort and improve quality of life.
Method: This is a pilot cross-sectional study developed at a Movement Disorders Outpatient Clinic at the northeast of Brazil. We included PD patients in the ON medication state, 18 years old or older, with no dementia (assessed by MMSE or MoCA). Patients presenting with other significant neurological disorders or those with deep brain stimulation (DBS) were excluded. Patients were assessed at two time points: an initial in-person evaluation using the Parkinson’s Disease Questionnaire (PDQ-8), Hospital Anxiety and Depression Scale (HADS), SE, and H&Y scales, along with the timed application of the KING and PD-PCS pain scales by two neurologists specializing in movement disorders. Follow-up evaluations are conducted via telemedicine, including PDQ-8, HADS, and KING and PD-PCS scores, with a minimum interval of 4 weeks, by a third evaluator specialized in pain.
Results: A total of 3 patients were included at this pilot study. Patient clinical profile is shown in Table 1. Regarding applicability, both scales were accepted, with a longer duration on PD-PCS application, as seen in table 1. PD-PCS showed a larger variation on the total score (from 42 to 142) which was not seen in the same patients regarding King’s final scores. This may be a considerable advantage when considering a scale that may be more sensible on clinical practice to follow-up pain treatment.
Conclusion: Preliminary descriptive analysis suggests a tendency for better PD pain assessment when using the PD-PCS, possibly with a higher sensitivity for identifying pain improvement or worsening on patient follow-up, even though longer application time may be needed.
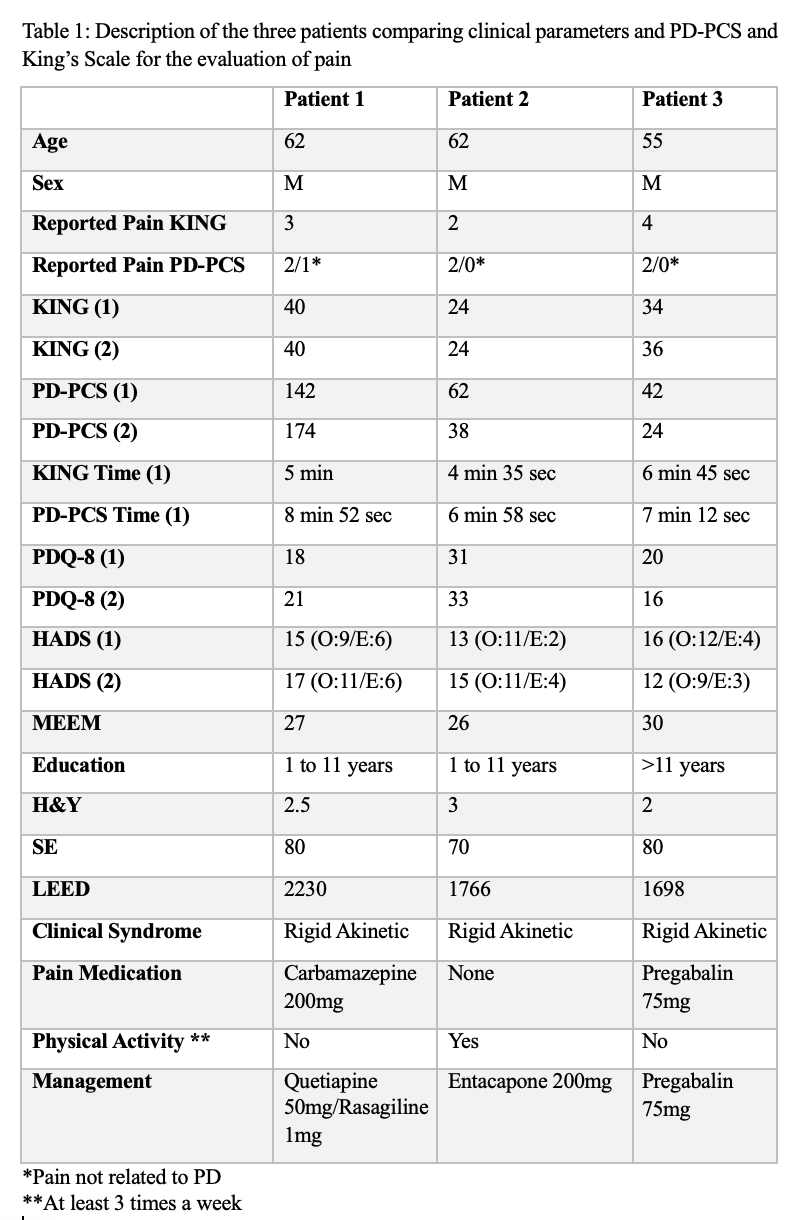
Table 1
References: 1. BEISKE, A. G. et al. Pain in Parkinson’s disease: Prevalence and characteristics. Pain, v. 141, n. 1–2, p. 173–177, jan. 2009.
2. CHAUDHURI, K. R.; SCHAPIRA, A. H. Non-motor symptoms of Parkinson’s disease: dopaminergic pathophysiology and treatment. The Lancet Neurology, maio 2009.
To cite this abstract in AMA style:
J. Queiroz, P. Matos, A. Ferreira Gomes, I. Santos, F. Rolim, D. de Andrade, F. Carvalho. Assessment of the Applicability of the King and PD-PCS Scales in Patients with Parkinson’s Disease and Chronic Pain: a Pilot Study [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/assessment-of-the-applicability-of-the-king-and-pd-pcs-scales-in-patients-with-parkinsons-disease-and-chronic-pain-a-pilot-study/. Accessed July 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/assessment-of-the-applicability-of-the-king-and-pd-pcs-scales-in-patients-with-parkinsons-disease-and-chronic-pain-a-pilot-study/