Category: Parkinson's disease: Neuroimaging
Objective: To assess if cardiovascular dysautonomia, evaluated by autonomic function tests (AFTs), is related to dopaminergic nicgrostriatal loss and other non-motor symptoms in early Parkinson disease (PD).
Background: The recent SOC model [1] proposes two different pathogenesis of PD, resulting in distinctive prodromal phase, “body-first vs brain-first”, affecting course and prognosis. The “body-first” variant would involve mainly autonomic structures, would be associated with prodromal Rem Behavior Disorder (RBD), hyposmia, more symmetric motor symptoms, more symmetric dopamine transporter loss. This hypothesis came from molecular imaging of sympathetic cardiac de-innervation, although often irrespective of clinical autonomic symptoms [2].
Method: Early levodopa-naïve PD patients were retrospectively included (LEDD<300 mg/die), with AFTs performed up to one year after 123I-FP-CIT-DAT-SPECT (DaTSCAN). Patients with any other condiction affecting autonomic nervous system were excluded. AFTs included cardiovascular reflexes (head-up tilt test HUTT, Valsalva maneuver, deep breathing, hand grip, and cold face). We considered as dysautonomic (PDys+) patients with neurogenic orthostatic hypothension or abnormal Valsalva or deep breathing measurment; the others as patients without dysautonomia (PDys-). Demographic and clinical variables, anamnestic data of hypo/anosmia, RBD, mood disorder and constipation were recorded. Mean striatal, putamen and caudate specifc binding ratios (SBR) and asymmetry index (AI) of putamen and caudate were computed. Student T-test and Mann-Whitney U test were used to compare groups, while chi-squared test for categorical variables.
Results: Twenty-four patients were included, 12 male and 12 female, mean age 58 ± 8 (6 PDys+ and 18 PDys-). Clinical and demographic variables were similar between groups. PDys+ showed a significant lower mean caudate-SBR (p=0.009). No significant differences in others mean SBR or AI were found [Figure 1]. Besides, PDys+ were associated with RBD (p=0,01), but not with the other non-motor features.
Conclusion: Dysautonomia in early PD is associated with higher dopaminergic loss of caudate region. This study showed similar asymmetry of dopaminergic pathways between PDys+ and PDys-, in contrast with the SOC model, but embrace literature evidence of a PD phenotype where dysautonomia is associated with RBD.
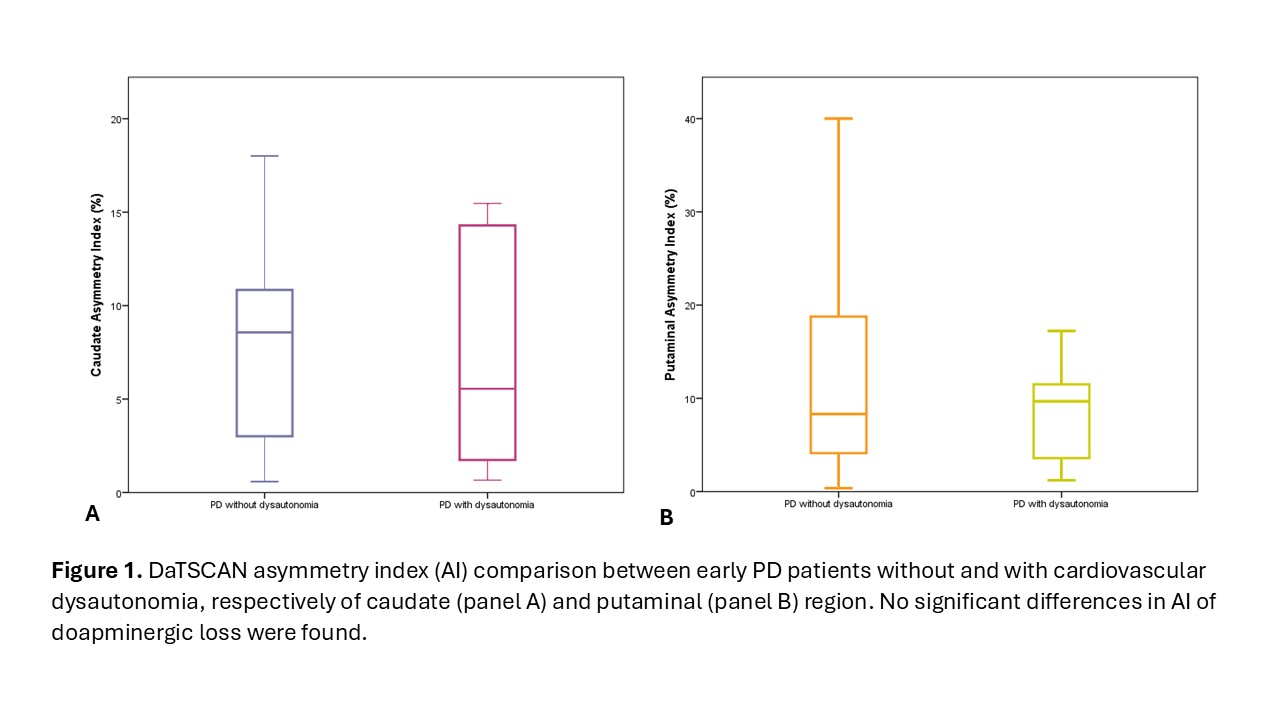
Figure 1
References: [1] Borghammer P. The α-Synuclein Origin and Connectome Model (SOC Model) of Parkinson’s Disease: Explaining Motor Asymmetry, Non-Motor Phenotypes, and Cognitive Decline. J Parkinsons Dis. 2021;11(2):455-474. doi: 10.3233/JPD-202481.
[2] Rocchi C, Pierantozzi M, Galati S, Chiaravalloti A, Pisani V, Prosperetti C, Lauretti B, Stampanoni Bassi M, Olivola E, Schillaci O, Stefani A. Autonomic Function Tests and MIBG in Parkinson’s Disease: Correlation to Disease Duration and Motor Symptoms. CNS Neurosci Ther. 2015 Sep;21(9):727-32. doi: 10.1111/cns.12437.
To cite this abstract in AMA style:
E. Garasto, A. Stefani, M. Pierantozzi, N. Mercuri, A. Chiaravalloti, C. Rocchi. Exploring the Association between Autonomic Responses and Dopaminergic Pathways in Early Parkinson’s Disease [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/exploring-the-association-between-autonomic-responses-and-dopaminergic-pathways-in-early-parkinsons-disease/. Accessed July 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/exploring-the-association-between-autonomic-responses-and-dopaminergic-pathways-in-early-parkinsons-disease/