Category: Spasticity
Objective: We present two HMS patients with distinct Doppler ultrasonography findings in the involved masseter muscle, however, both responded favorably to botulinum toxin A injections.
Background: Hemimasticatory spasm (HMS) is an uncommon disorder characterized by paroxysmal spasms or twitches of the unilateral jaw-closing muscles [1]. Treatment options include botulinum toxin injection, microvascular decompression, masseteric nerve avulsion, and pharmacological therapy [2].
Method: Case 1
A 43-year-old man presented with a 13-year history of episodic involuntary muscle contractions and painful spasms in his left cheek. Twitching contractions of the right masseter muscle were observed on examination along with hypertrophy of the left masseter and temporalis muscles (Fig. 1A). Doppler ultrasonography showed the maximum thickness of the masseter muscle was greater on the left (Fig. 1C) than the right (Fig. 1D). Botulinum toxin A was injected into his left masseter (50 U) and temporalis (10 U). At the 1-month follow-up, the left masseter muscle hypertrophy was improved(Fig. 1B) and the frequency of the spasms had decreased to once every 8 to 10 days.
Case 2
A 34-year-old man presented with a 4-year history of involuntary contractions of the left jaw and difficulty in mouth-opening. On physical examination, the left masseter muscle appeared normal in size. However, when the patient was asked to clench his teeth, involuntary contraction of the left masseter was observed. On Doppler ultrasonography, the left masseter muscle appeared normal at rest (8.4 mm vs 10.9 mm, Fig. 2A and 2B) ; however, it considerably increased in muscle thickness during contraction (18.3 mm, Fig. 2C), particularly when compared with the right side (14.6mm, Fig. 2D). MRI of the brain showed vascular compression of the left trigeminal nerve (Fig. 2E). The patient was injected with botulinum toxin A (50 U) into the left masseter. One month after treatment, he reported significant relief from the spasms without residual discomfort.
Results: Both patients, including one with vascular compression of the trigeminal nerve, experienced a good response to botulinum toxin injections without side effects.
Conclusion: Despite of the etiology, clinical and imaging diversity of HMS, botulinum toxin injections remain the most effective treatment. Doppler ultrasonography is an economical and valuable tool for evaluating patients with HMS, providing insight into muscle activity at rest and during contraction.
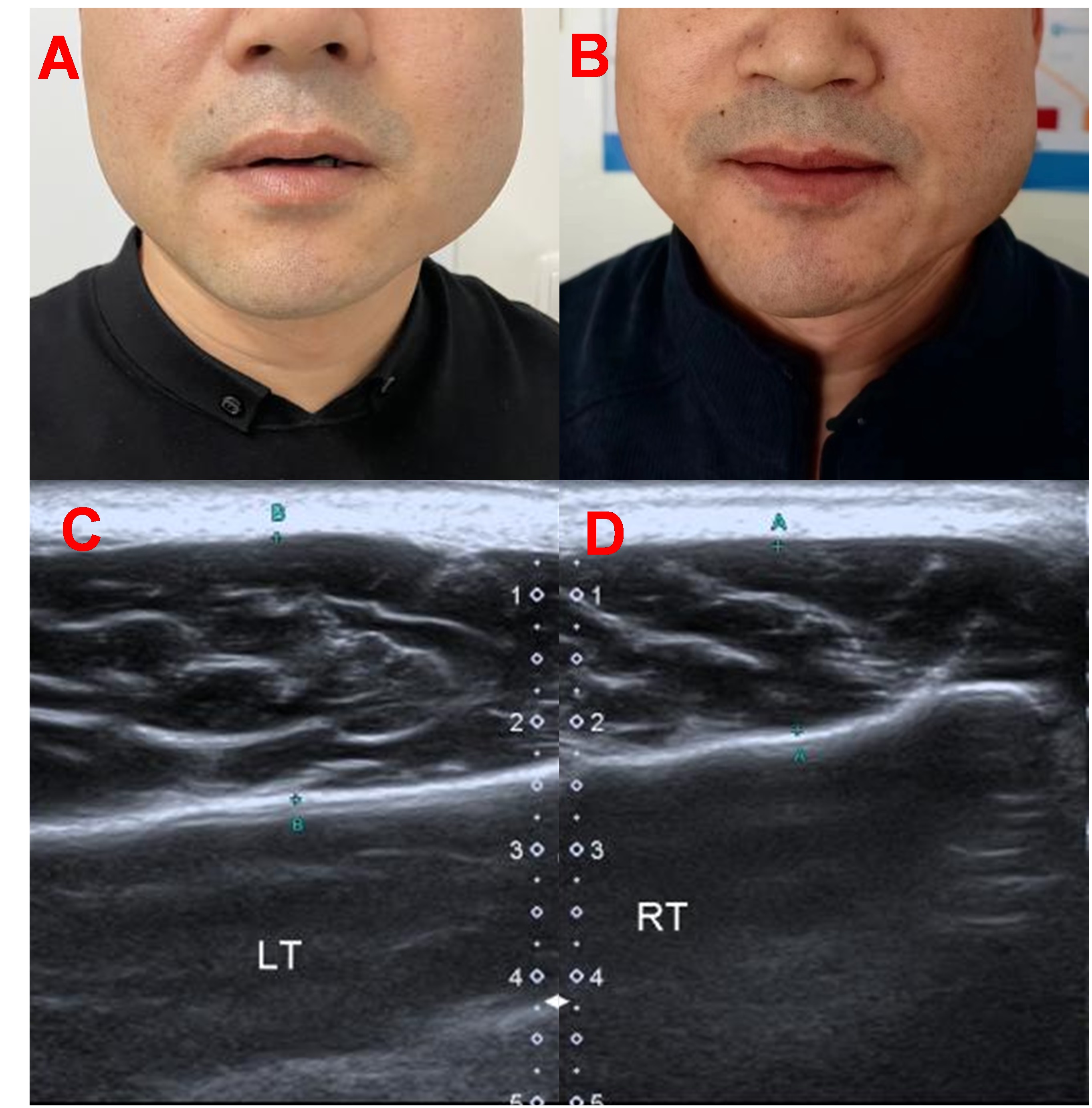
Fig. 1 Case 1.
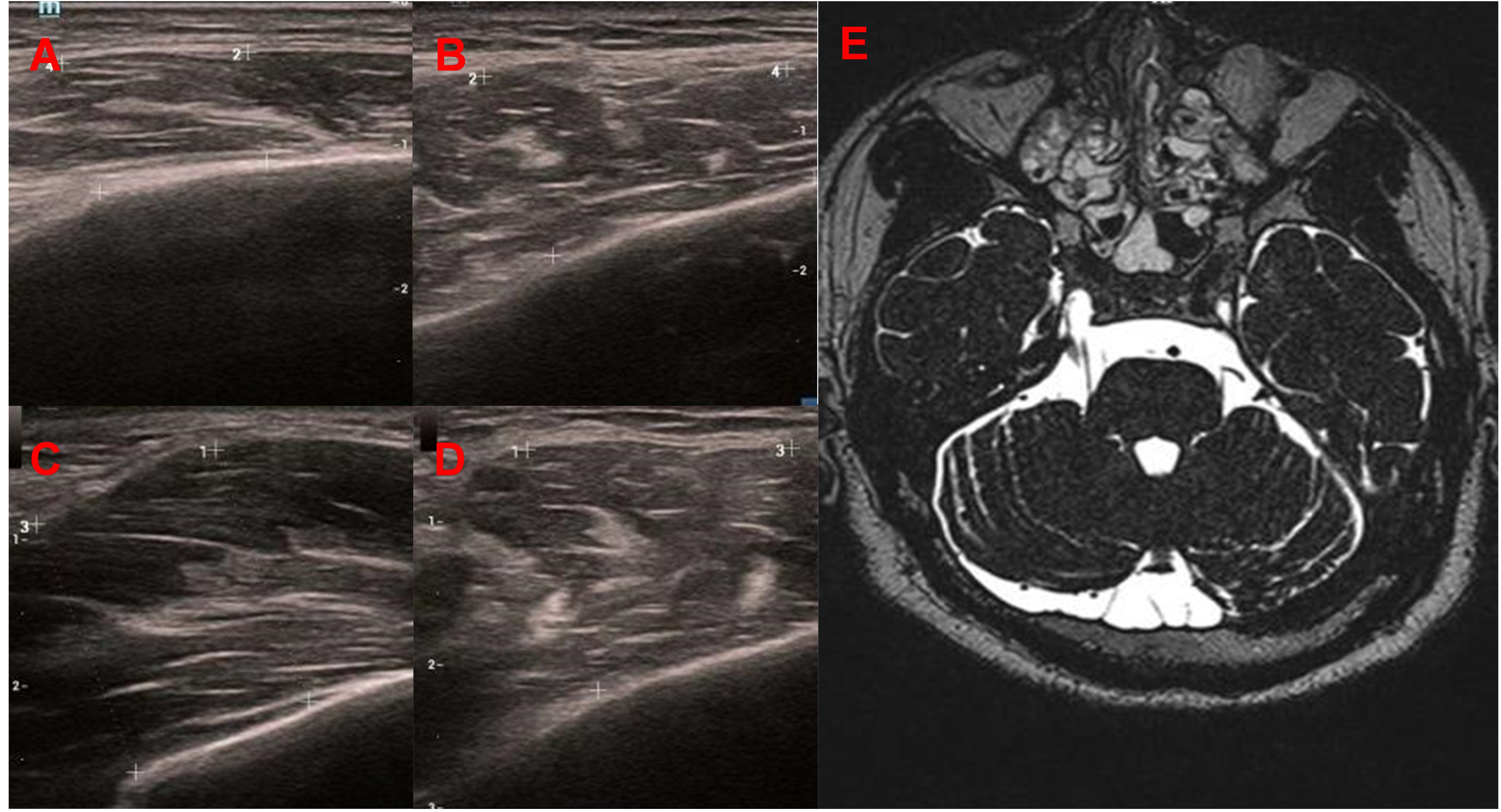
Fig. 2 Case 2.
References: 1. Thompson PD, Carroll WM. Hemimasticatory and hemifacial spasm: a common pathophysiology? Clin Exp Neurol. 1983;19:110-9.
2. Li Q, Wang X, Wang L, et al. Surgical treatment strategies for hemimasticatory spasms. Chin Med J (Engl). 2022;135(9):1105-7.
To cite this abstract in AMA style:
X. Xing, N. Ren, . Tang, L. Chen. Hemimasticatory Spasm: A Report of Two Cases [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/hemimasticatory-spasm-a-report-of-two-cases/. Accessed July 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/hemimasticatory-spasm-a-report-of-two-cases/