Category: Dystonia: Genetics
Objective: To study the clinical course, imaging and genetics in a case of early onset generalized dystonia with suspected Neurodegeneration with Brain Iron Accumulation (NBIA).
Background: Pantothenate Kinase-associated Neurodegeneration (PKAN) is a type of NBIA caused by mutations (commonly c.1561G>A) in the Pantothenate Kinase 2 (PANK2) gene.1 Classic PKAN has an earlier age of onset (1st or 2nd decade) and rapid progress. 1
Method: An 8-year-old boy, the first-born child of healthy and consanguineous parents from West India, presented with gradually progressing abnormal posturing of bilateral feet, with difficulty in walking, first noticed by parents at around 4 years of age. This was followed by abnormal postures of both hands, abnormal posturing of neck and trunk with arching of spine and dystonic jerk of trunk and recurrent falls. He also developed involuntary movements of the eyes, jaw and tongue. He exhibited gradual language regression, mental and intellectual retardation, such that he could not speak even simple words like “baba” and “mama”, and was bed-bound. However, no difficulty in swallowing or any psychiatric symptoms were noted. No family history relevant was obtained.
Upon ophthalmic examination, Kayser- Fleischer ring was absent and fundi were normal. Intermittent oculogyric crisis was noted. Amongst other significant positive findings, blepharospasm, jaw-opening dystonia, lingual dystonia, left rotacollis, opisthotonus postering of the trunk and dystonic posturing of both UL and LL was noted. Brisk DTR and extensor planter responses were observed (Fig1).
Results: Routine investigations and slit lamp examination were normal. His T2WMRI showed ‘eye -of- the- tiger’ sign (Fig2) and iron accumulation in SWI. Typical PKAN was suspected because of the rapidly progressive generalized dystonia and the typical radiological sign. So, genetic testing for PANK2 mutation was pursued.
Clinical exome sequencing revealed homozygous mutations in exon 6 (c.1267dup p.Leu423ProfsTer33- Depth-53x) in the PANK2 gene (Fig3). This case report, to the best knowledge of the author, is the first report of this frameshift variant c.1267dup (p.Leu423ProfsTer33) in the PANK2 gene, i.e. a novel genetic variation.
Conclusion: The author reports a novel homozygous mutation causing PKAN, absent in gnomAD exomes, adding a new PKAN causing mutation in genomic library for future work.

Figure-1: Phenomology: Generalized Dystonia
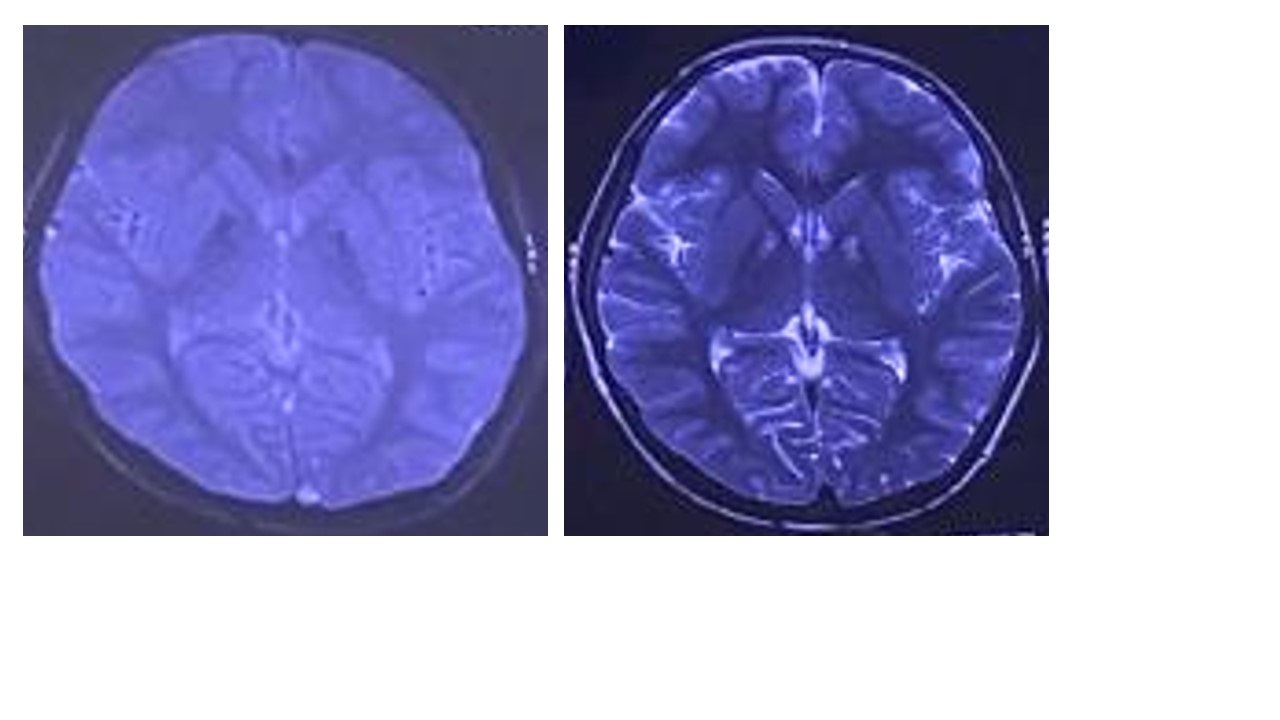
Eye-of-the-tiger sign on T2WI;hypointensity on SWI
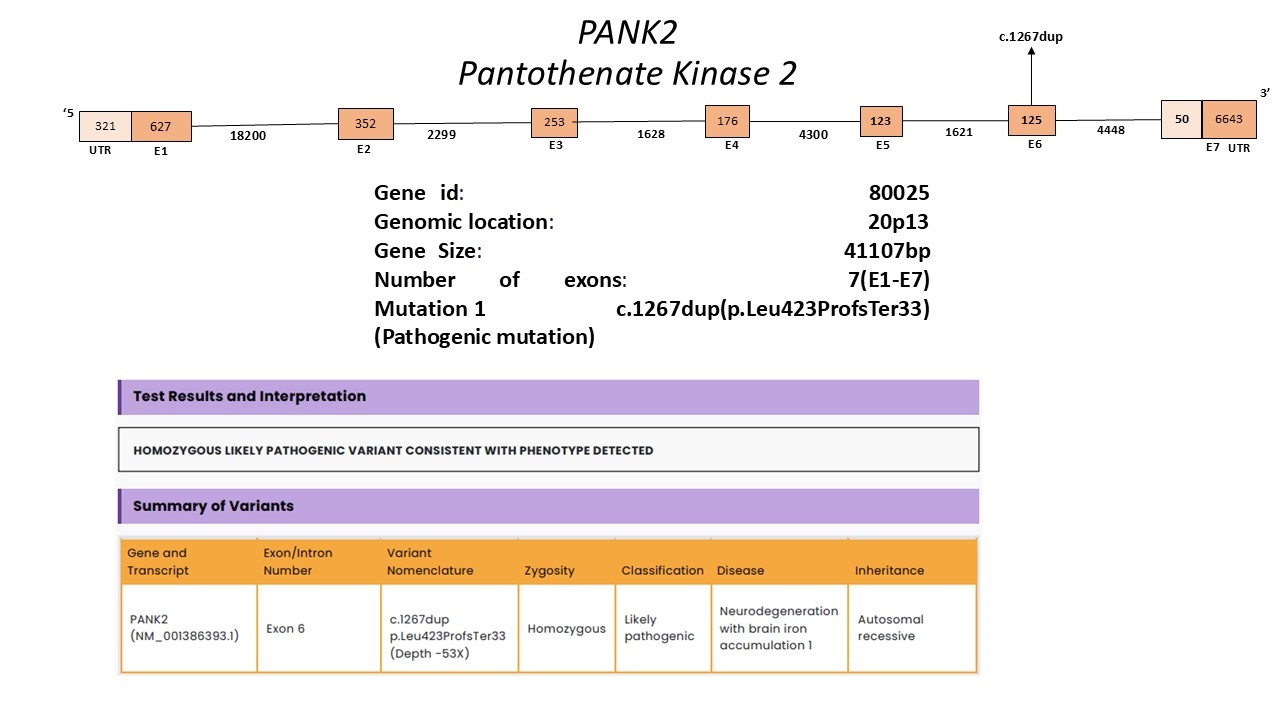
Genetic report showing novel PANK2 mutation
References: 1. Kurian MA, Hayflick SJ. Pantothenate kinase-associated neurodegeneration (PKAN) and PLA2G6-associated neurodegeneration (PLAN): review of two major neurodegeneration with brain iron accumulation (NBIA) phenotypes. Int Rev Neurobiol. 2013;110:49-71. doi:10.1016/B978-0-12-410502-7.00003-X
To cite this abstract in AMA style:
H. Chovatiya. A novel homozygous mutation in PANK2 gene mutation in a South- Asian male with typical PKAN [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/a-novel-homozygous-mutation-in-pank2-gene-mutation-in-a-south-asian-male-with-typical-pkan/. Accessed April 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/a-novel-homozygous-mutation-in-pank2-gene-mutation-in-a-south-asian-male-with-typical-pkan/