Objective: To describe the clinical, radiological, laboratory and genetic findings of a patient with Cerebrotendinous Xanthomatosis (CTX) who presented with dystonic tremor initially and subsequently developed dystonia of the lower limbs.
Background: A 26 year old caucasian female presented with a 7 year history of progressively worsening tremor, and worsening eyesight. Tremor was bilateral, asymmetrical and had a jerky appearance, a null point, and mirror dystonia. Dystonia of the lower limbs was evident when walking, with prominent abduction at the hip on the right. Cognitive function was normal.
Additional features included thickened Achilles tendons and bilateral cataracts.
Method: Patient underwent Computed Tomography (CT) scan of the brain, with and without contrast, followed by Magnetic Resonance Imaging (MRI) brain.
Thin-Layer Chromatography (TLC) was done on silica gel G on a sterol extract.
Genetic analysis was carried out with the Dystonia panel provided by Invitae (San Francisco, CA).
Dystonia was assessed using the Abnormal Involuntary Movement Scale (AIMS) and Unified Dystonia Rating Scales (UDRS).
Ox bile was prescribed at a dose of 500 mg twice daily.
Results: Contrasted CT brain showed moderate generalized cerebral atrophy only, confirmed on MRI.
Genetic testing revealed a pathogenic variant in the CYP27A1 gene (c.850A>T (p.Lys284*) (nonsense mutation exon 5), and a missense mutation in exon 4 of the CYP27A1 gene (c.667G>C (p.Glu223Gln) ,currently classified as a VUS (variant of uncertain significance).
TLC showed three bands, corresponding to the polar sterols 7-OH cholesterol, Δ4-3-one, and 3β,5α,6β-cholestanetriol (the latter a probable marker for CTX). No cholestanol band was observed with TLC.
At baseline, AIMS score was 17 and UDRS 17.5. Four months following treatment AIMS and UDRS had improved to scores of 9 and 8 respectively.
Conclusion: This patient was diagnosed with CTX, with relatively mild neurological features. Imaging revealed only moderate cerebral atrophy. She is presumed to be a compound heterozygote with a pathogenic nonsense mutation in exon 5 of the cholesterol 27 hydroxylase (CYP27) gene and a missense mutation in exon 4. Use of over the counter bile salts resulted in improvement of the condition in this patient, and may be an alternative to chenodeoxycholic acid, in cases where the drug is costly or not available.
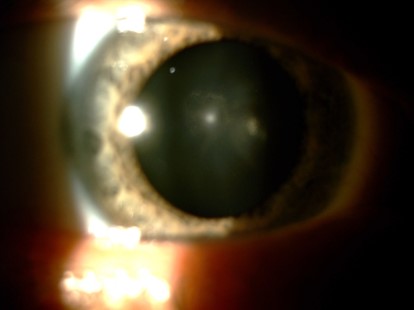
Bilateral cataracts were present.

Tendon xanthomas of the Achilles tendons
References: 1. Barkhof F, Verrips A, Wesseling P, van Der Knaap MS, van Engelen BG, Gabreëls FJ, Keyser A, Wevers RA, Valk J. Cerebrotendinous xanthomatosis: the spectrum of imaging findings and the correlation with neuropathologic findings. Radiology. 2000 Dec;217(3):869-76. doi: 10.1148/radiology.217.3.r00dc03869. PMID: 11110956.
To cite this abstract in AMA style:
N. de Jong, J. Carr, D. Marais. Cerebrotendinous Xanthomatosis successfully treated with Chenodeoxycholic Acid Supplementation [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/cerebrotendinous-xanthomatosis-successfully-treated-with-chenodeoxycholic-acid-supplementation/. Accessed April 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/cerebrotendinous-xanthomatosis-successfully-treated-with-chenodeoxycholic-acid-supplementation/