Category: Non-Dystonia (Other)
Objective: To present a unique case of adult-onset opsoclonus-myoclonus ataxia plus demyelinating neuropathy syndrome in a patient with large cell neuroendocrine prostate carcinoma with isolated anti-neurofascin antibodies.
Background: Opsoclonus-myoclonus ataxia syndrome (OMAS) is a rare neurologic condition, characterized by opsoclonus and myoclonic jerks, ataxia, irritability, and sleep disturbance. OMAS is less common in adults than in children. In adults, the cause is usually suspected to be immune-mediated, paraneoplastic, or idiopathic. Most adult cases have been associated with breast adenocarcinoma or small cell lung cancer [1]. Very few descriptions have been found of OMAS associated with prostate cancer [2-4].
Method: Case report
Results: A 69-year-old male, diagnosed with metastatic large cell neuroendocrine carcinoma of the prostate, developed nausea, vomiting, dizziness, and unsteadiness triggered by changes in position. Initially diagnosed with vestibular neuritis, but symptoms progressed over a few months, with gait instability and behavioral changes. A brain MRI with and without contrast was unremarkable [figure 1]. He was noted to have a combination of macro-saccadic oscillations in his eye movements, tremulousness and myoclonic jerks consistent with OMAS. Electromyography (EMG) of the left extremities showed mild hyperacute demyelinating neuropathy. Cerebrospinal fluid analysis was remarkable for elevated proteins, negative paraneoplastic antibody panel but serum demyelinating neuropathy panel resulted positive for IgM and IgG antibodies against Neurofascin-186, IgG against neurofascin-155 and 140. DOTATE PET scan showed active metastatic disease [figure 2]. He underwent a 5-day course of IVIG, followed by 5 days of IV methylprednisolone, and then transitioned to weekly IV steroid treatments for 12 weeks with improvement of symptoms and EMG findings.
Conclusion: Among paraneoplastic causes of OMAS, prostate cancer is an uncommon association. This is the first case of OMAS described in association with large cell neuroendocrine prostate carcinoma with demyelinating neuropathy syndrome and isolated anti-neurofascin antibodies. An upfront immunosuppressive therapy with both IVIG and IV steroids seemed to be effective for this case, knowing that OMAS has been described to have worse prognosis when a paraneoplastic etiology is associated.
Figure 1
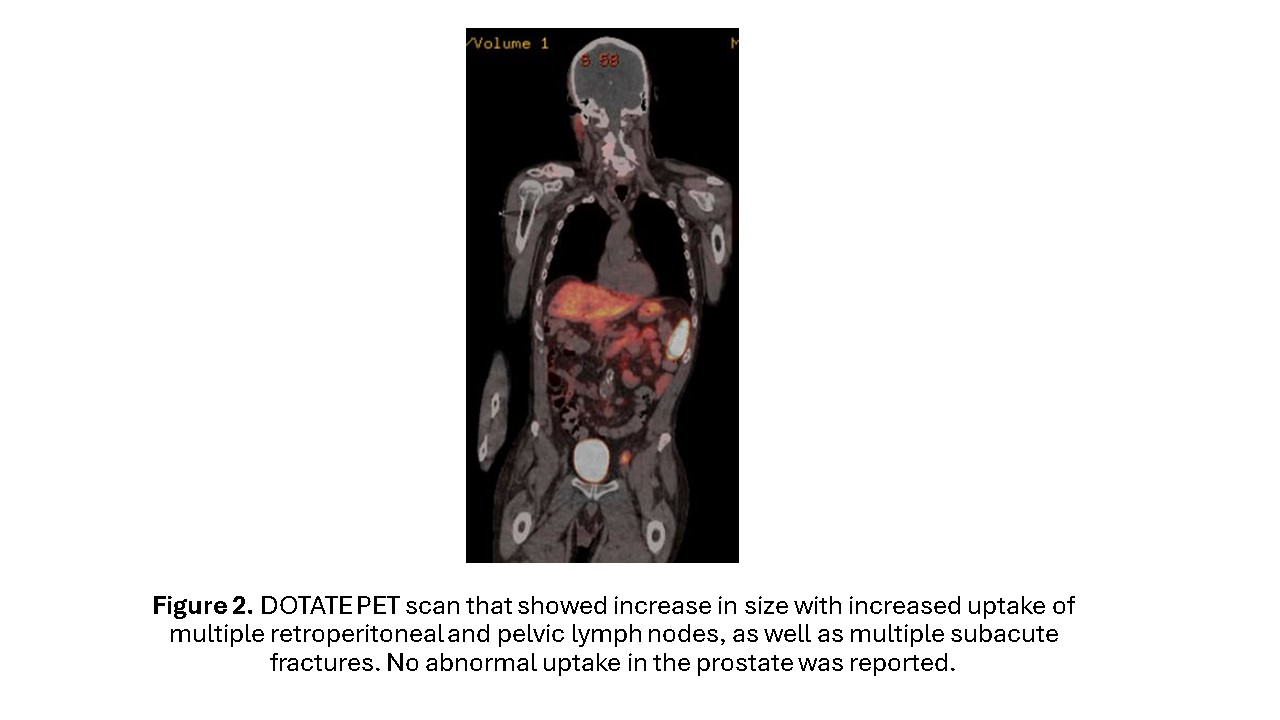
Figure 2
References: [1] Klaas JP, Ahlskog JE, Pittock SJ, et al. Adult-Onset Opsoclonus-Myoclonus Syndrome. Arch Neurol. 2012;69(12):1598–1607. doi:10.1001/archneurol.2012.1173
[2] Fromowitz A, Sharma R, Nissenblatt M, Copeland T. Paraneoplastic Opsoclonus-Myoclonus Syndrome and Prostate Cancer: First Reported Case (2463). Neurology. 2020 Apr 15;94(15_supplement): 2463.
[3] Cuenca Hernández R, Esquivel Lopez A, Gordo Mañas R, Hípola González D. Benign opsoclonus myoclonus syndrome and prostate cancer. Neurologia (Engl Ed). 2020 Jan-Feb;35(1):64-65. English, Spanish. doi: 10.1016/j.nrl.2017.07.015. Epub 2017 Sep 25. PMID: 28958399.
[4] Guijarro-Castro C, Estallo-Guijarro L. Opsoclonus-myoclonus syndrome and prostate cancer. An entity to be aware of. Neurologia (Engl Ed). 2024 Feb 20:S2173-5808(24)00042-7. doi: 10.1016/j.nrleng.2024.02.004. Epub ahead of print. PMID: 38387776.
To cite this abstract in AMA style:
V. Parra Payano, N. Ahmed, M. Situ Kcomt. Opsoclonus-Myoclonus Ataxia plus Demyelinating Neuropathy Syndrome in an uncommon type of Prostate Cancer, a Case Report [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/opsoclonus-myoclonus-ataxia-plus-demyelinating-neuropathy-syndrome-in-an-uncommon-type-of-prostate-cancer-a-case-report/. Accessed April 12, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/opsoclonus-myoclonus-ataxia-plus-demyelinating-neuropathy-syndrome-in-an-uncommon-type-of-prostate-cancer-a-case-report/