Objective: To test whether PD risk is greater in those with a prior diagnosis of T2DM, and whether T2DM is associated with faster PD clinical progression.
Background: T2DM has been increasingly associated with greater risk of PD.[1] Faster progression has also been reported, but data are limited.[2] A causal association is biologically plausible. In addition to effects on glucose metabolism, T2DM has a diverse range of physiological effects on neurons and glia, including reduced mitochondrial Complex I activity, oxidative stress, inflammation and protein aggregation.
Method: As part of an ongoing study, we investigated a cohort of 146,776 veterans who utilized VA healthcare between 1999-2021.[3] We identified those with an ICD code for PD (332.0, G20) in outpatient, inpatient, or community care settings, and validated PD diagnosis and incidence date by record review. We defined T2DM as >= 2 ICD codes (250.x0, 250.x2, E11.x), at least one of which preceded PD diagnosis. We tested associations of T2DM and PD risk using a nested case-control design, matching 10 controls to each veteran with PD on age at diagnosis (“index date”), gender, race, and rank. We adjusted conditional logistic regression models for camp, smoking, and duration of VA usage prior to index date. With follow up through February 2021, we tested whether time until psychosis (earliest of diagnosis or antipsychotic medication), a diagnosis of fall or fracture, or time until death was shorter in PD cases with T2DM vs. PD cases without T2DM using Cox regression models.
Results: We identified a total of 430 veterans with PD, 259 (60.2%) of whom used VA healthcare prior to PD diagnosis [table1]. In the nested substudy, prevalence of T2DM was 26.3% in those with PD and 18.9% in 2515 matched controls (adjusted odds ratio (aOR) 1.62, 95%CI 1.40-1.87, p<0.0001) [table2]. Risk was higher in women, but estimates were imprecise. Among all veterans with PD, the adjusted risks of psychosis and death were modestly but non-significantly increased in those with T2DM [table3][figure1][figure2].
Conclusion: These results add to a growing body of evidence that implicates T2DM as a risk factor for PD and a potential modifier of PD progression. Given its high population prevalence and potential modifiability, further elucidation of the mechanisms underlying the association of T2DM and PD is essential.
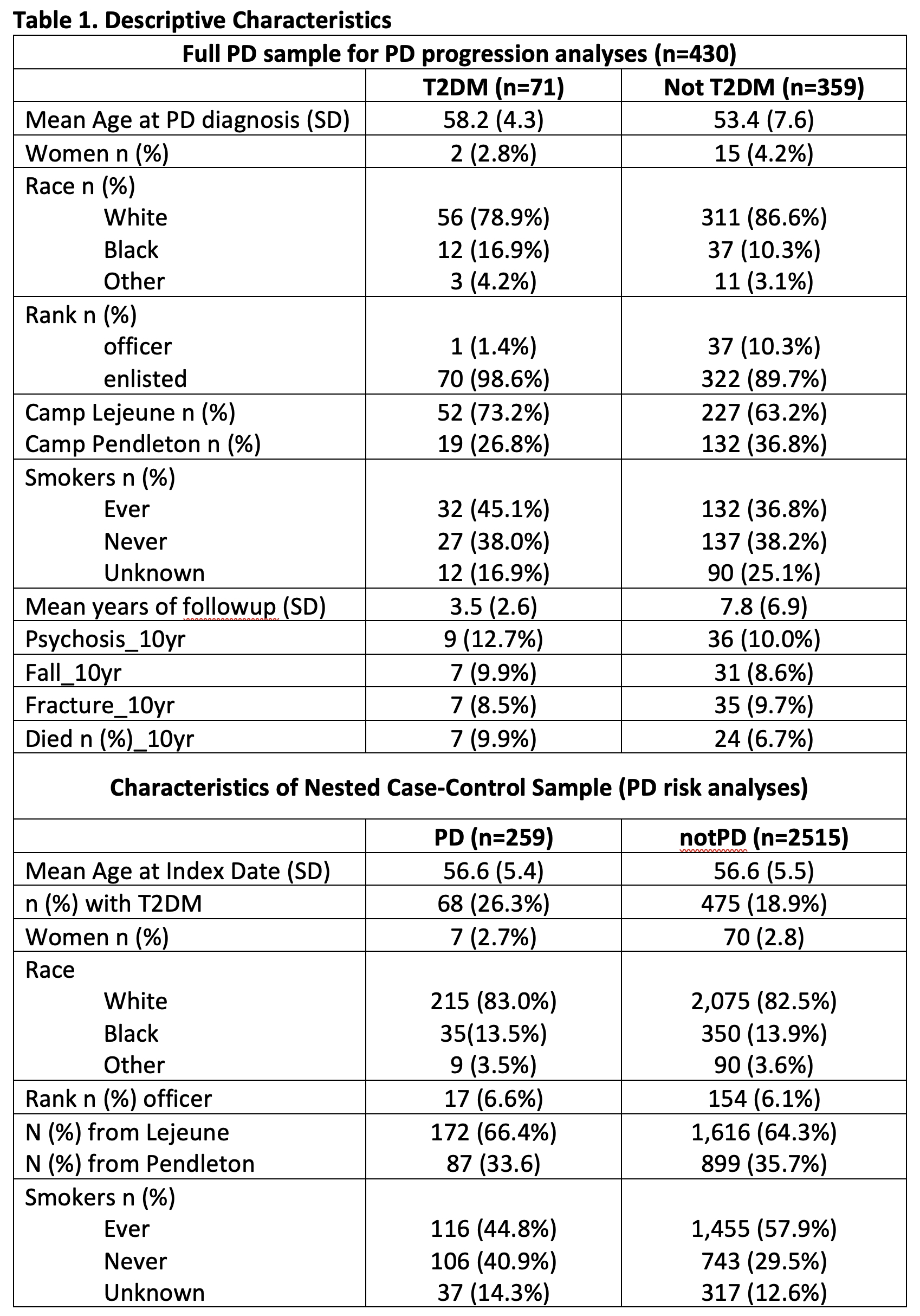
Table 1
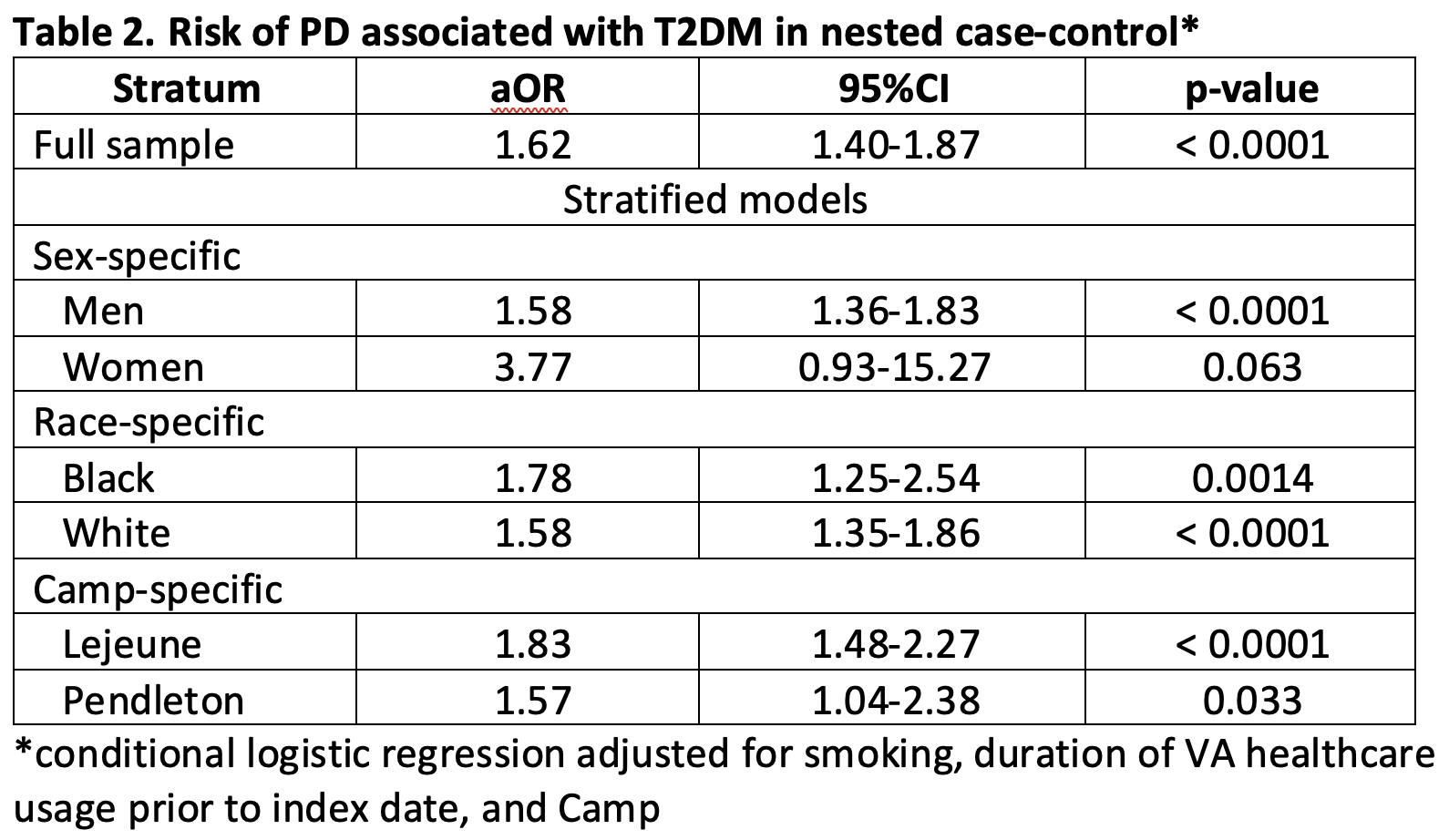
Table 2
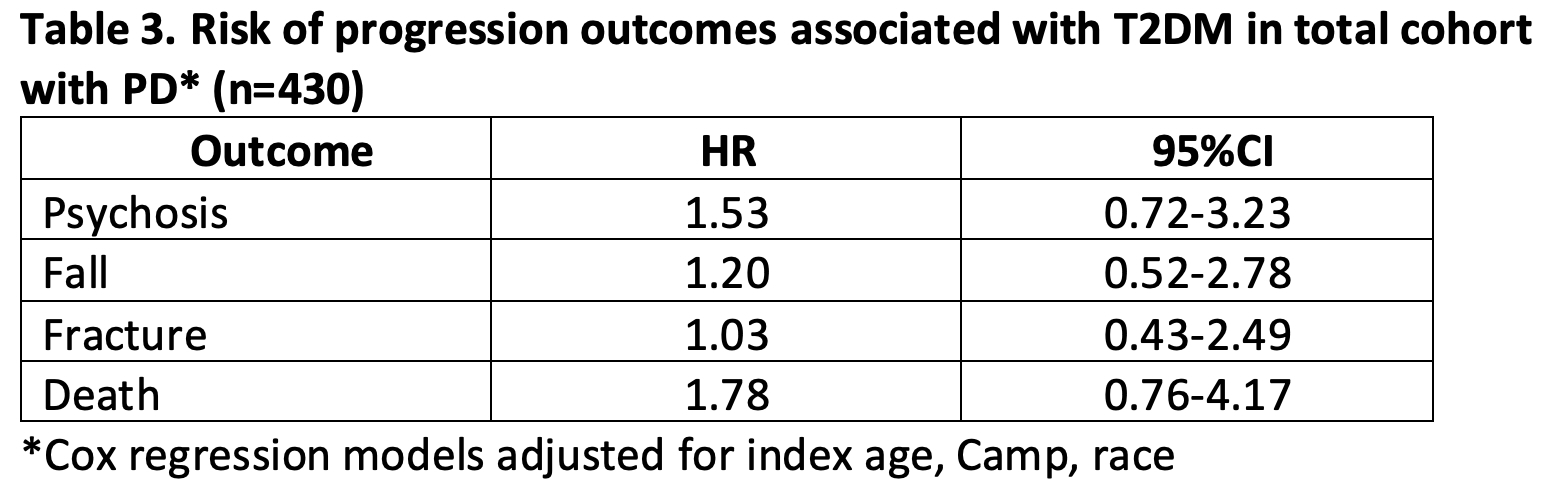
Table 3
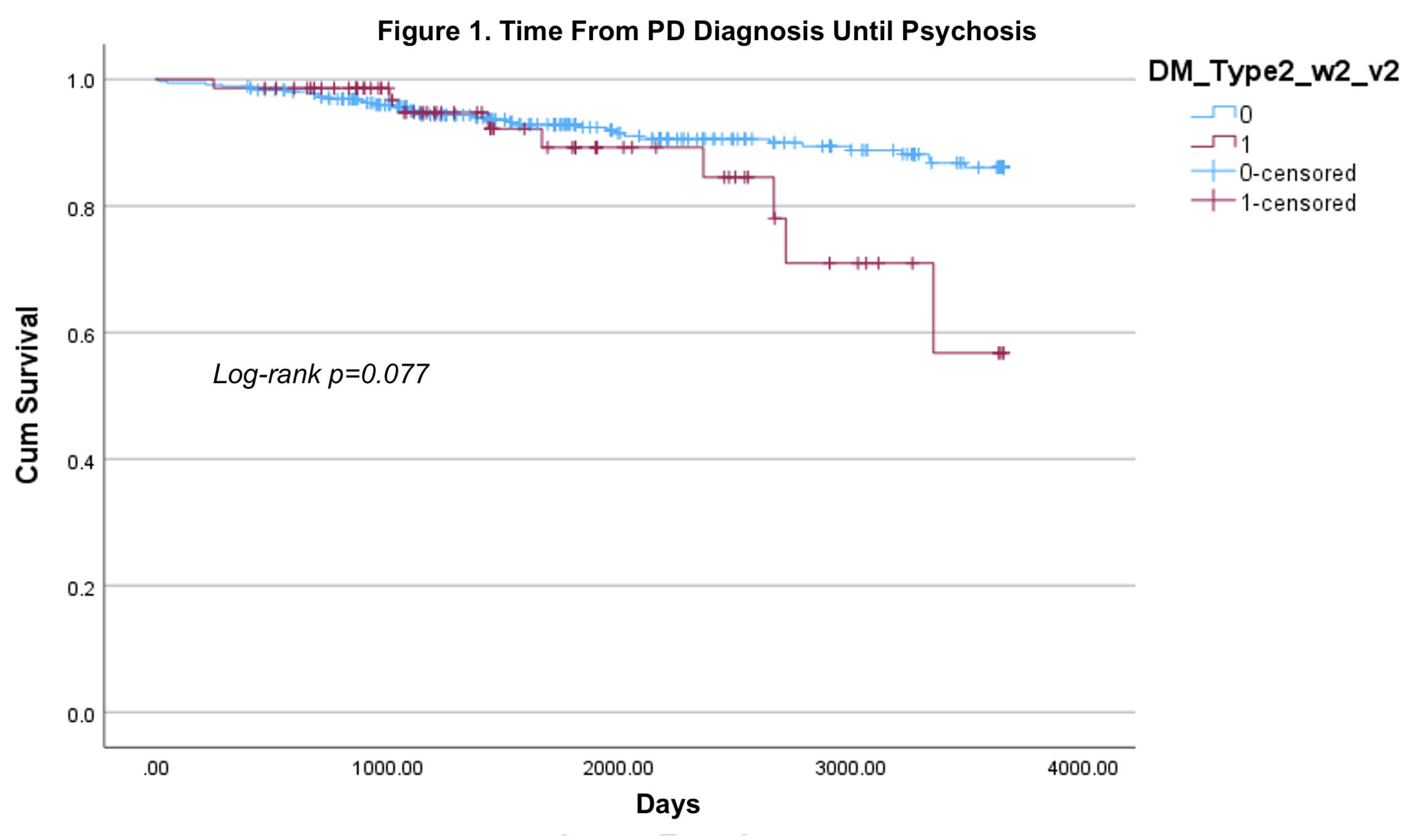
Figure 1
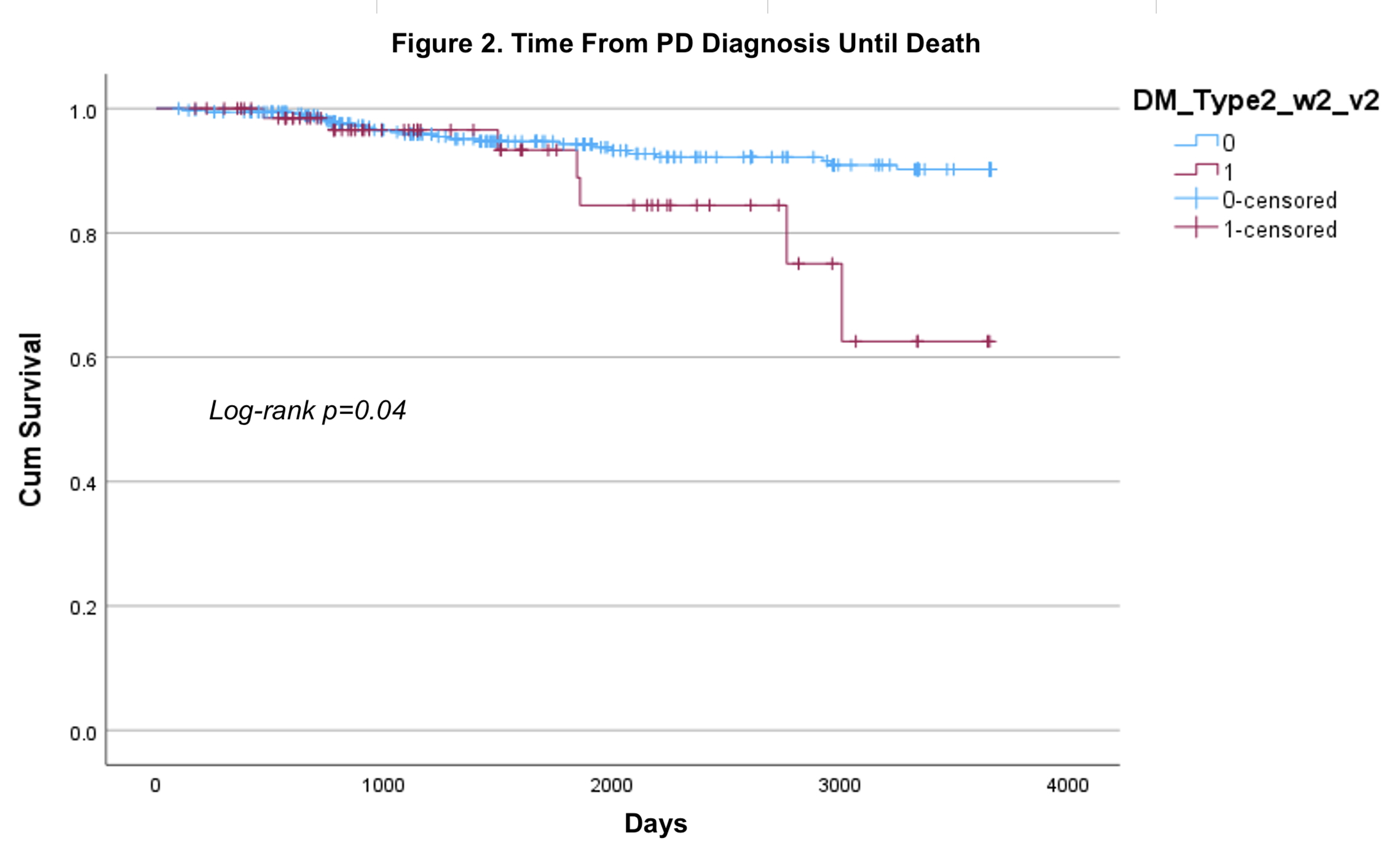
Figure 2
References: 1. Cullinane PW, de Pablo Fernandez E, Konig A, Outeiro TF, Jaunmuktane Z, Warner TT. Type 2 Diabetes and Parkinson’s Disease: A Focused Review of Current Concepts. Mov Disord. 2023 Feb;38(2):162-77.
2. Athauda D, Evans J, Wernick A, Virdi G, Choi ML, Lawton M, Vijiaratnam N, Girges C, Ben-Shlomo Y, Ismail K, Morris H, Grosset D, Foltynie T, Gandhi S. The Impact of Type 2 Diabetes in Parkinson’s Disease. Mov Disord. 2022 Aug;37(8):1612-23.
3. Goldman SM, Weaver FM, Stroupe KT, Cao L, Gonzalez B, Colletta K, Brown EG, Tanner CM. Risk of Parkinson Disease Among Service Members at Marine Corps Base Camp Lejeune. JAMA Neurology. 2023 Jul 1;80(7):673-81.
To cite this abstract in AMA style:
S. Goldman, F. Weaver, L. Cao, B. Gonzalez, S. Jugnundan, K. Stroupe, K. Colletta, E. Brown, C. Tanner. Parkinson’s Disease (PD) and Type II Diabetes (T2DM): Risk and Progression [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/parkinsons-disease-pd-and-type-ii-diabetes-t2dm-risk-and-progression/. Accessed April 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/parkinsons-disease-pd-and-type-ii-diabetes-t2dm-risk-and-progression/