Category: Parkinsonism, Others
Objective: To report the clinical features of a patient with Perry syndrome (PS) due to a heterozygous novel pathogenic variant in the DCTN1 gene.
Background: PS is a rare autosomal dominant neurodegenerative disorder mainly characterized by the combination of parkinsonism, refractory depression/apathy, respiratory symptoms, and weight loss. Less frequently frontal signs, oculomotor disturbances, or cognitive impairment can also be present [1]. DCTN1 mutations as the cause of PS were first described in 2009. All but two described mutations are located in a “hot spot”, the CAP-Gly domain (exon 2 between amino acids 48 and 90). There is high phenotypic variation between mutations located in the same domain [2], so we consider genotype and phenotype correlations of new DCTN1 gene mutations should be reported.
Method: A 74-year-old woman with no familiar history of parkinsonism or psychiatric disturbances, presented to our institution with a year history of slowness of movements and difficulties performing tasks with her right arm, frequent backward falls, non-quantified significant weight loss, and depressed mood. At physical examination, asymmetric parkinsonism without oculomotor abnormalities and freezing of gait was detected. No respiratory complaints were noticed at that moment. Levodopa treatment was started up to 600mg/d with no improvement. DATSCAN showed no reduction of striatal tracer uptake. MRI and FDG-PET were unremarkable.
Polysomnography was performed then revealing severe obstructive sleep apnea with an apnea-hypopnea index of 47.1 and also whole exome sequencing, revealing a novel heterozygous DCTN1 mutation (NM_004082.5:c. 259A>G; Ile87Val). PS was diagnosed according to current criteria [3]. At this moment patient is alive and has denied the use of ventilatory aids.
Results: This new variant (DCTN1 Ile87Val) lies within the “hot-spot” CAP-Gly domain in a patient with the PS phenotype [Figure 1]. According to in silico prediction [4], this new variant appears to be pathogenic (CADD, PolyPhen-2, and SIFT score of 23.8, 0.97, and 0.02, respectively). Applying the ACMG-AMP criteria for the interpretation of sequence variants [5], it is likely pathogenic (PM1, PM6, PP2, PP3, PP4).
Conclusion: Apart from the cardinal features of PS, early postural instability appears to be one of the main features of this Ile87Val DCTN1 mutation, but further reports are needed to confirm this, as this is a single case report.
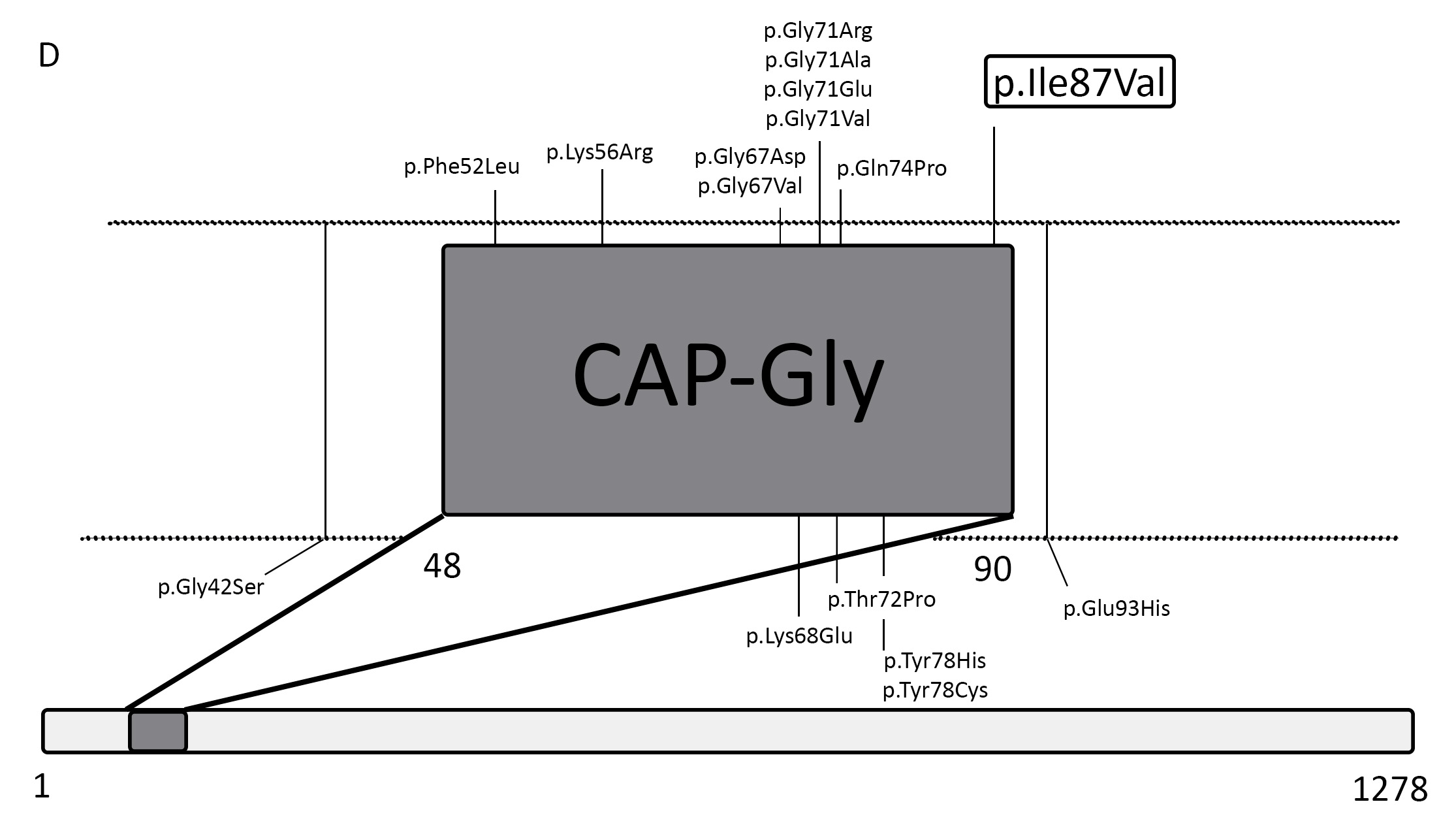
DCTN1 mutations reported in Perry Syndrome to date
References: 1. Dulski J, Cerquera-Cleves C, Milanowski L, et al. Clinical, pathological and genetic characteristics of Perry disease—new cases and literature review. Eur J Neurol. 2021;28(12):4010-4021. doi:10.1111/ene.15048
2. Konno T, Ross OA, Teive HAG, Sławek J, Dickson DW, Wszolek ZK. DCTN1-related neurodegeneration: Perry syndrome and beyond. Parkinsonism Relat Disord. 2017;41:14-24. doi:10.1016/j.parkreldis.2017.06.004
3. Mishima T, Fujioka S, Tomiyama H, et al. Establishing diagnostic criteria for Perry syndrome. J Neurol Neurosurg Psychiatry. 2018;89(5):482-487. doi:10.1136/jnnp-2017-316864
4. Martin FJ, Amode MR, Aneja A, et al. Ensembl 2023. Nucleic Acids Res. 2023;51(1 D):D933-D941. doi:10.1093/nar/gkac958
5. Richards S, Aziz N, Bale S, et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genetics in Medicine. 2015;17(5):405-424. doi:10.1038/gim.2015.30
To cite this abstract in AMA style:
P. Lorenzo-Barreto, I. Muro-García, E. Casas-Peña, JP. Romero-Muñoz, L. López-Manzanares. Perry Syndrome due to a DCTN1 novel variant [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/perry-syndrome-due-to-a-dctn1-novel-variant/. Accessed June 30, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/perry-syndrome-due-to-a-dctn1-novel-variant/