Objective: We describe a case of a 66-year-old woman who developed cervical dystonia with dystonic tremor and hypertrophic olivary degeneration (HOD) after a right pontine hemorrhage.
Background: The patient presented with left sided numbness and weakness, diplopia, and dysphagia, and was found to have a hypertensive right pontine hemorrhage. Approximately 4 weeks following the event, the patient developed a new tremor of the head, neck, and right (unaffected) arm.
Method: Over the next few months, she had improvement in the dysphagia and left-sided weakness with persistent left sided numbness. The head tremor persisted, and trials of propranolol, levetiracetam, and carbidopa-levodopa offered no therapeutic benefit. Swallowing notably improved with changes in head position, especially turning the head to the left. It seemed her head and neck tremor contributed to the swallowing difficulty.
Results: The patient’s repeat brain MRI 4 months after the initial hemorrhage showed interval improvement in the hemorrhage and brainstem edema without an underlying mass. However, there was subsequent development of bilateral HOD (figure 1), more prominent on the right. Examination 5 months after the initial presentation showed a primarily horizontal head tremor, mild right torticollis, slight left laterocollis, slight left shoulder elevation, and mild retrocollis. Null point was achieved with turning the head fully in either direction, though more persistently suppressed with head turn to the left. There was also a low frequency postural tremor in the right arm that became most prominent in the wing-beating position. There were a few beats of uvular tremor noted when her mouth and palate were at rest. The option of botulinum toxin injections was considered, and after a detailed discussion of the risks, benefits, and alternatives with the patient, especially the risk of worsening baseline dysphagia, a joint decision was made to proceed cautiously with injections which yielded slight benefit without side effects and repeat injections were planned.
Conclusion: Bilateral HOD is a known complication of lesions involving the brainstem, including hemorrhage. Palatal tremor and dystonia are known manifestations of HOD, but to our knowledge, this is first report of cervical dystonia and dystonic tremor as the principal movement disorders associated with these changes.
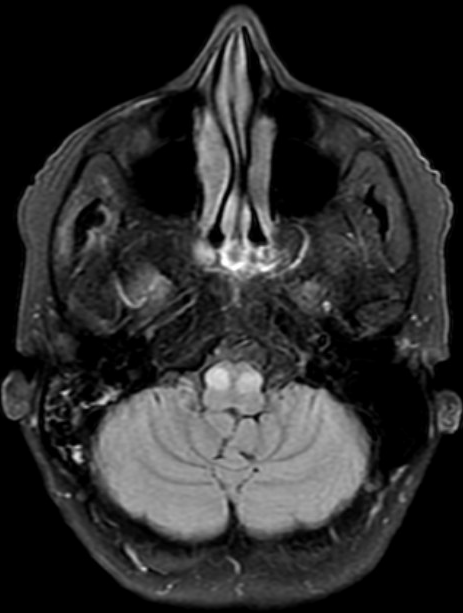
figure 1
To cite this abstract in AMA style:
M. Iqbal, C. Tarolli, D. Manou. Pontine Hemorrhage leading to Bilateral Olivary Degeneration and Cervical Dystonia [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/pontine-hemorrhage-leading-to-bilateral-olivary-degeneration-and-cervical-dystonia/. Accessed April 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/pontine-hemorrhage-leading-to-bilateral-olivary-degeneration-and-cervical-dystonia/