Category: Myoclonus/Tics/Stereotypies
Objective: To describe a rare presentation of propriospinal myoclonus (PSM) restricted to upper cervical segments and discuss the diagnostic challenge posed by its overlap with functional movement disorders (FMDs).
Background: PSM is a rare movement disorder originating in the spinal cord, causing involuntary, flexor arrhythmic jerks of the trunk, hips, and knees, often stimulus sensitive and increased when supine. Diagnosing PSM is challenging due to overlap with FMDs. Atypical presentations, such as focal upper extremity jerks from upper cervical involvement, are exceedingly rare. Rapid symptom resolution with low-dose clonazepam blurs distinction from FMDs.
Method: A 56-year-old male with alcohol use presented with acute positional involuntary upper extremity and neck movements when lying down, resolving upon sitting or standing. Neurological examination and work-up was performed to identify the cause of PSM.
Results: Examination revealed large-amplitude, arrhythmic upper extremity jerks when supine during wakefulness. Movements were non-suppressible, non-distractible, with occasional lower extremity jerks, sparing head and neck muscles. There was bilateral hyperreflexia and foot clonus in the lower extremities, without rigidity, bradykinesia, tremors, or facial/vocal involvement. Labs were unremarkable. CT head and MRI cervical/thoracic-spine showed no abnormalities, making this likely idiopathic PSM. Symptoms resolved after two doses of 0.5 mg clonazepam, without recurrence during hospitalization, further blurring distinction from FMDs.
Conclusion: This case illustrates a rare PSM presentation restricted to upper cervical segments, causing jerks in the shoulders and upper extremities while sparing head, neck, and lower extremities. Clinicians should consider PSM in patients with positional (supine) myoclonic jerks for accurate diagnosis and management. Such focal presentations may mimic FMDs, especially when symptoms rapidly resolve with low-dose clonazepam. The lack of specific biomarkers complicates differentiation from FMDs. Evaluation for structural etiology (seen in 7% of PSM) in the cervical spinal cord is important (secondary PSM). Polymyography is considered an essential diagnostic procedure. Features include a fixed pattern of muscle activation, slow spinal cord conduction (5–15 m/d), and no involvement of facial muscles. The absence or presence of Bereitschaftspotential may help distinguish PSM from FMDs.
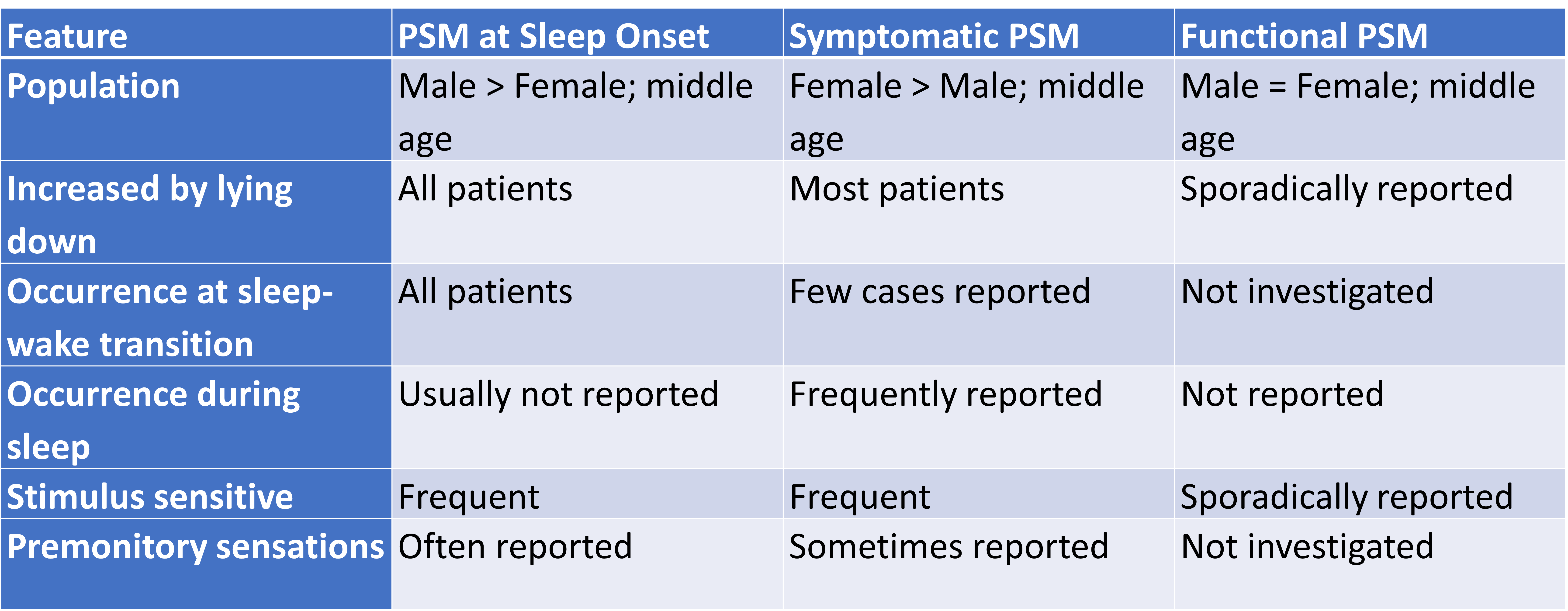
Table 1
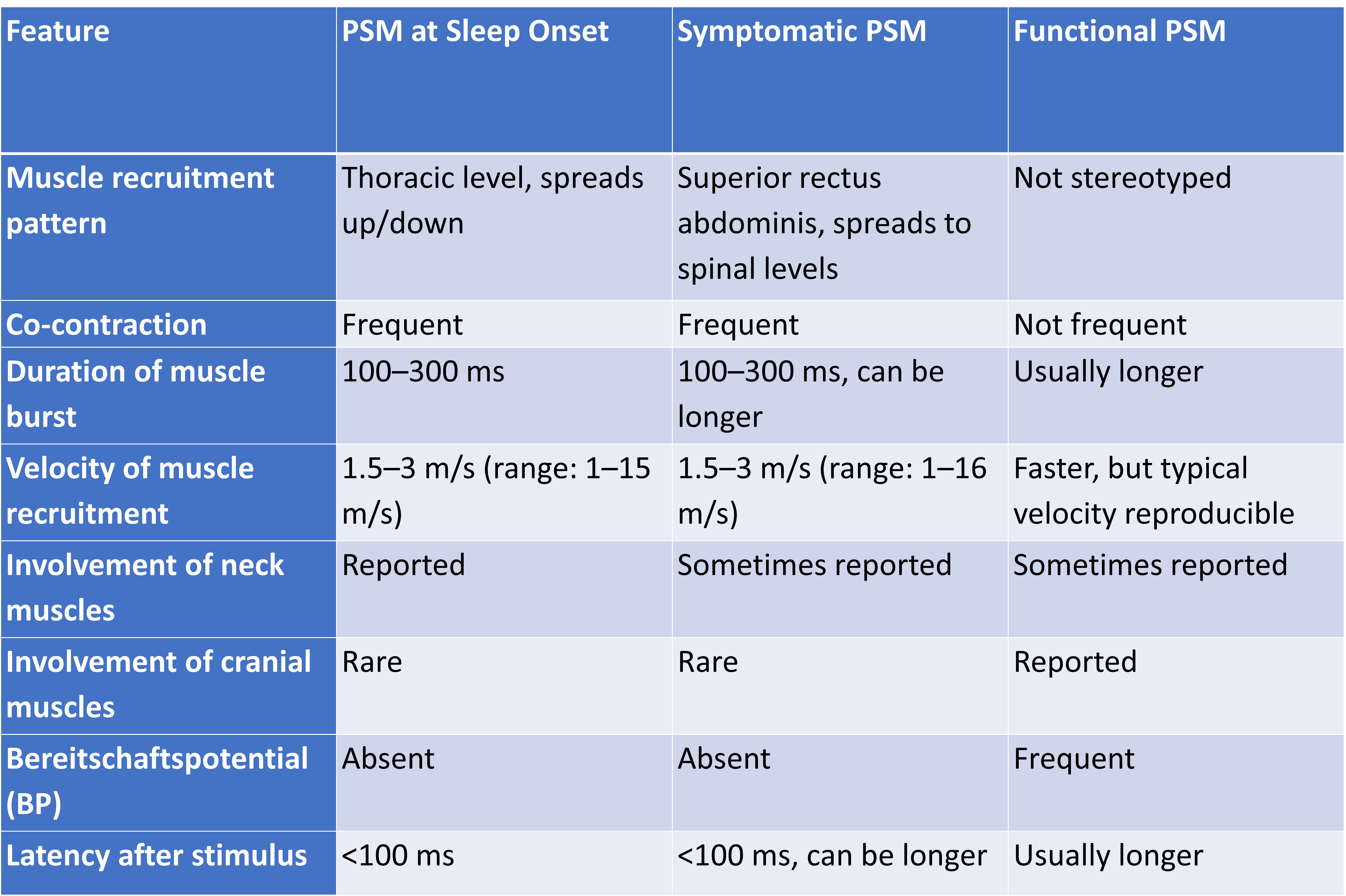
Table 2
References: Brown P, Thompson PD, Rothwell JC, Day BL, Marsden CD. Axial Myoclonus of Propriospinal Origin.
Termsarasab P, Thammongkolchai T, Frucht SJ. Spinal-generated movement disorders: a clinical review. J Clin Mov Disord. 2015 Dec;2(1):18.
Erro R, Bhatia KP, Edwards MJ, Farmer SF, Cordivari C. Clinical diagnosis of Propriospinal Myoclonus is unreliable: An electrophysiologic study. Movement Disorders. 2013 Nov;28(13):1868–73.
Manconi M, Sferrazza B, Iannaccone S, Massimo A, Zucconi M, Ferini‐Strambi L. Case of symptomatic Propriospinal Myoclonus evolving toward acute “myoclonic status.” Movement Disorders. 2005 Dec;20(12):1646–50.
Antelmi E, Provini F. Propriospinal Myoclonus: The spectrum of clinical and neurophysiological phenotypes. Sleep Medicine Reviews. 2015 Aug;22:54–63.
Thomsen BLC, Teodoro T, Edwards MJ. Biomarkers in Functional Movement Disorders: a systematic review. J Neurol Neurosurg Psychiatry. 2020 Dec;91(12):1261–9.
Roze E, Bounolleau P, Ducreux D, Cochen V, Leu-Semenescu S, Beaugendre Y, et al. Propriospinal Myoclonus revisited: Clinical, neurophysiologic, and neuroradiologic findings. Neurology. 2009 Apr 14;72(15):1301–9.
To cite this abstract in AMA style:
S. Khurana, A. Prabhu. Shaking, Not Stirred: An Atypical Case of Propriospinal Myoclonus [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/shaking-not-stirred-an-atypical-case-of-propriospinal-myoclonus/. Accessed April 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/shaking-not-stirred-an-atypical-case-of-propriospinal-myoclonus/