Category: Dystonia: Clinical Trials and Therapy
Objective: To report a Wilson disease patient (WD) with subacute combined degeneration (SCD) from zinc and D-penicillamine.
Background: Copper-lowering treatments are main strategies to reduce copper excess due to impaired hepatic copper transport in WD. However, overtreatment can result in copper deficiency. SCD from WD treatment have rarely been reported in the literature, and poses challenges in treatment.
Method: Case report
Results: A 46-year-old woman, diagnosed with WD at age 23, initially presented with generalized dystonia and dysarthria, Kayser-Fleischer rings, low serum ceruloplasmin, and high 24-hour urine copper. Initial treatment with D-penicillamine offered partial improvement. Botulinum toxin injections led to moderate improvement of cervical dystonia. Zinc was added 3 years ago, aiming for a transition to zinc-only maintenance therapy. In recent follow-up visits, she was on D-penicillamine 1000 mg/d and zinc 100 mg/d. She complained of numbness in hands and feet, unsteady gait and falls for 3 months. Examination revealed hypertonia, hyperreflexia, impaired proprioception and vibration with preserved pinprick sensation in bilateral legs, hyperesthesia in both hands, and positive Romberg sign. Serum copper was <10 μg/dL, and 24-hour urine copper was 70 μg/dL. Serum vitamins B12 and E were normal. EMG showed axonal polyneuropathy. Spinal MRI showed a long T2 hyperintense signal in the dorsal column from C1-T1 levels (Figure 1), confirming SCD. Discontinuation of zinc led to partial improvement. Discontinuation of D-penicillamine led to marked improvement 1 month later. The plan is to monitor 24-hour urine copper levels and resume treatment once they exceed 500 μg/dL.
Conclusion: This patient highlights SCD from overtreatment of WD with both D-penicillamine and zinc. While copper reduction is the main treatment strategy, overtreatment may lead to copper deficiency. To prevent or detect SCD early, careful clinical and laboratory monitoring, including 24-hour urine copper, is essential. Delayed detection and treatment can result in poor outcomes. Managing such cases is complex, since copper-lowering therapies need to be withheld. It is critical to closely monitor to identify the optimal timing for resuming WD therapies. This case underscores the therapeutic dilemma of balancing the administration and withholding of copper reduction in WD. A literature review will be presented.
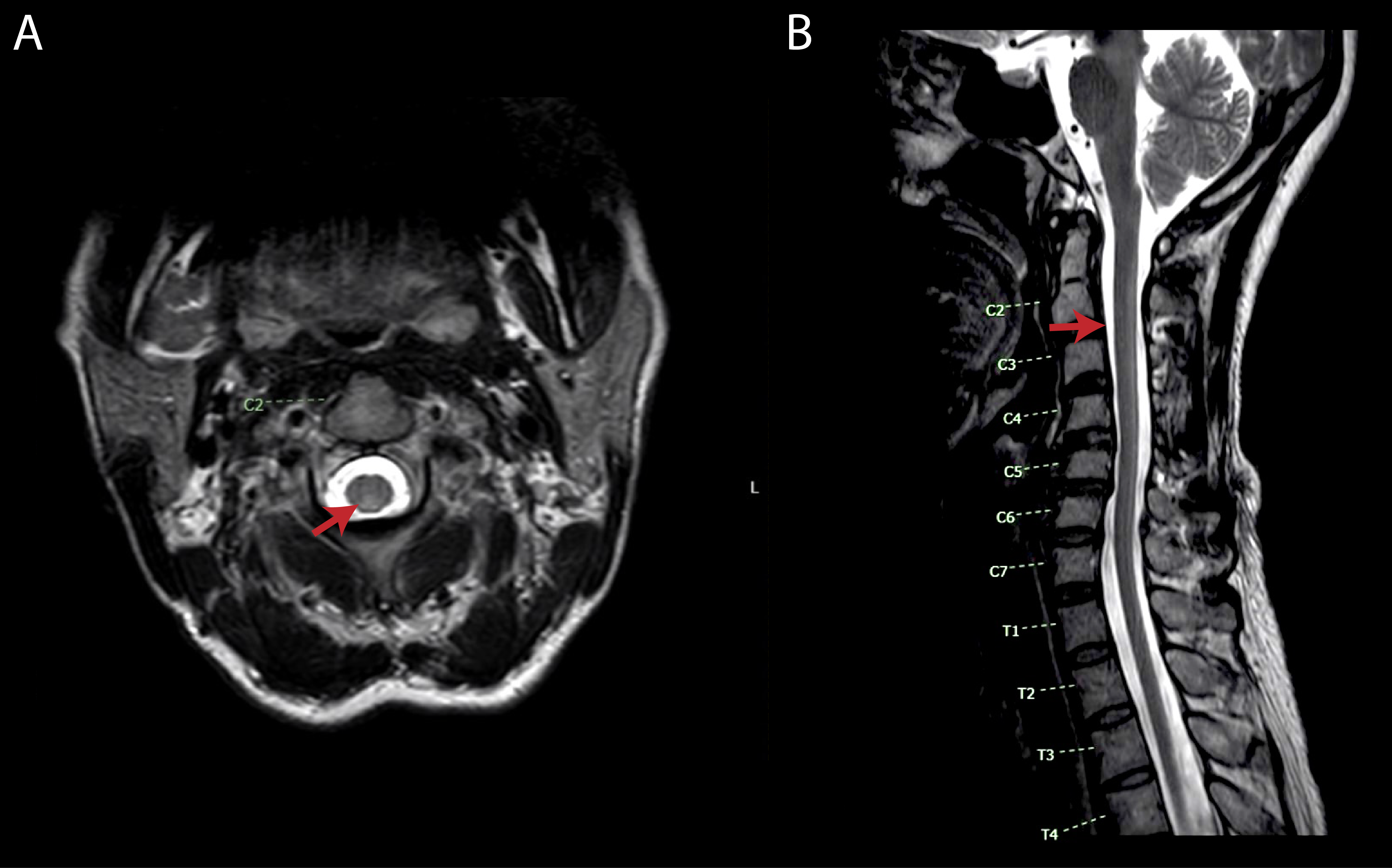
Figure 1
To cite this abstract in AMA style:
T. Thammongkolchai, P. Termsarasab. Subacute Combined Degeneration in Wilson Disease: Treatment Dilemma [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/subacute-combined-degeneration-in-wilson-disease-treatment-dilemma/. Accessed July 21, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/subacute-combined-degeneration-in-wilson-disease-treatment-dilemma/