Objective: It may be difficult to distinguish the reason of previously described symptoms in case of acute comorbidities accompanying Parkinson’s disease
The 69 y.o. man was hospitalised in ICU. He had a previous history of PD with rare episodes of visuospatial disorders. The patient was space and time disoriented, stayed up all night, fidgeted.
Background: The patient has 7 years history of PD AR form with episodes of illusions and hallucinations. His condition was decompensated after long-distance trip in the train (4 hours). He regularly took levodopa drugs (750 mg daily). Also he take 10 mg dosage of apixaban usually due to atrial fibrillation.
Method: The CT found the haemorrhage in right parahippocampal gyrus area. The MRI found signs of triventricular hydrocephalia.
Results: At first the patient received levodopa-carbidopa 125 mg 6 times per day. After each dose of the drug we witnessed deterioration of the patient’s condition – psychomotor agitation increased. An increase in rigidity occurred, so we had to continue the levodopa therapy. We had to add atypical antipsychotic therapy (clozapine 25 mg per day). After than the patient was calm, friendly, answered questions, identified himself and oriented in space properly, though disoriented in time. However, the increase in rigidity remained. Due to the need of antipsychotic therapy and insufficient effect of levodopa drugs we added Amantadine (PK-Merz) infusions (200 mg) – 2 per day. The amantadine infusion lasted approximately 4 hours a day during 3 days with simultaneous dynamic monitoring of the patient’s condition. We revealed positive dynamics: significant reduction of movement impairment, stabilization of consciousness with less amount of psychomotor destabilization. No increase in visuospatial disorders frequency occurred during combination of Amantadine and Levodopa due to plateau of Clozapine concentration and positive dynamics of hematoma resolution. After the course of infusions we changed the therapy – added amantadine 400 mg PO with positive effect on the gait and movements. After 6 months ventriculoperitoneal shunting was made with positive effect on the gait, balance and cognition
Conclusion: This case shows the role of comorbide pathologies which can both decompensate PD and be the reason of similar symptoms. When assessing existing symptoms, progression/decompensation of the disease, concomitant and possible competing pathology should be considered
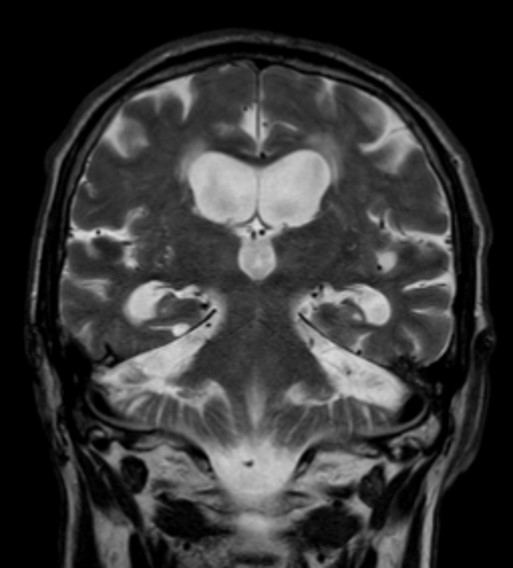
Triventricular hydrocephalia on MRI
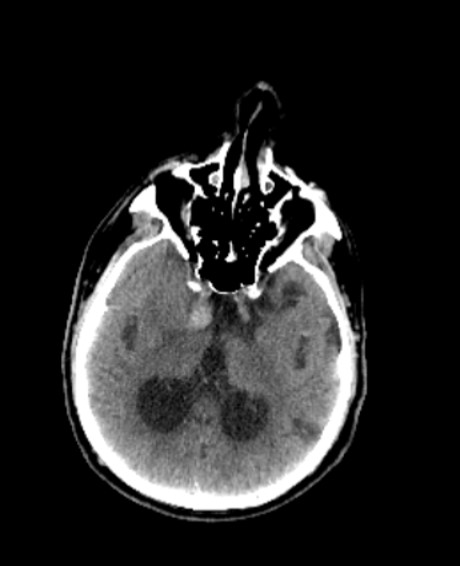
Right parahyppocampal gyrus haemorrhage on CT
References: Aminoff EM, Kveraga K, Bar M. The role of the parahippocampal cortex in cognition. Trends Cogn Sci. 2013 Aug;17(8):379-90. doi: 10.1016/j.tics.2013.06.009. Epub 2013 Jul 10. PMID: 23850264; PMCID: PMC3786097.
To cite this abstract in AMA style:
P. Dynin, V. Yakovleva. The Clinical Case of Acute Comorbidities in Parkinson’s Disease [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/the-clinical-case-of-acute-comorbidities-in-parkinsons-disease/. Accessed April 6, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/the-clinical-case-of-acute-comorbidities-in-parkinsons-disease/