Objective: Characterize clinical features of dystonia and levodopa-related dyskinesias in Parkinson disease (PD).
Background: Dystonia affects 30-60% of individuals with PD. [1] Despite recognition as a debilitating symptom, there has been minimal efforts to elucidate PD-related dystonia pathophysiology, and how it differs from other dystonia phenotypes and levodopa-related motor complications. Identifying specific clinical features in PD-related dystonia is an essential first step for developing targeted therapies.
Method: Participants with PD were selected from two longitudinal studies that include cognitive testing, video-recorded motor assessments, and a clinical interview on their symptoms including presence of dystonia. Two analyses of variance (ANOVA), one comparing individuals with PD with and without dystonia, and the other with and without dyskinesias were performed. Dependent variables included age, age at time of diagnosis, duration of PD motor symptoms and Levodopa Equivalent Daily Dose (LEDD). Chi-square tests were used to compare the proportion of categorical variables between groups including sex and presence of anxiety or depression symptoms.
Results: 191 participants with PD (40% female) provided data on presence or absence of dystonia. Among those, 120 (63%) reported dystonia, 70 (35%) dyskinesias, and 47 (25%) both symptoms. Individuals with dystonia (p<0.001) and those with dyskinesias (p=0.03) were significantly younger at the time of PD motor symptom onset than those without. Duration of motor symptoms, time since PD diagnosis, and LEDD were not associated with presence of dystonia, but were strongly associated with levodopa-related dyskinesias (p<0.001) [figure1]. There were no differences based on sex, or presence of anxiety or depression symptoms [figure2].
Conclusion: The high prevalence and association with younger age at onset match previous literature and restate the dimension and impact of dystonia in PD. [1,2] Lack of sex differences and comorbid anxiety or depression symptoms differs from epidemiological data in isolated focal dystonia. [3,4] Absence of an association with disease duration or LEDD distinguishes dystonia from levodopa-related dyskinesias in PD. These findings suggest a unique pathophysiology for PD-dystonia. Future directions include analyzing functional neuroimaging in this same cohort to identify dystonia-specific functional connectivity patterns underlying this debilitating symptom.
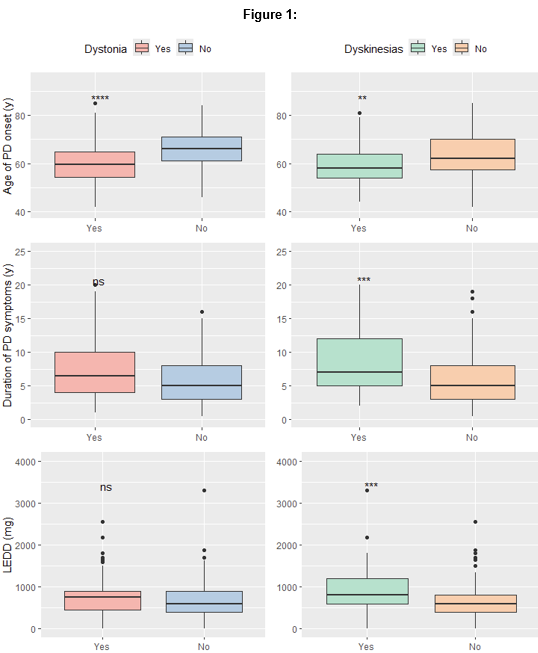
Figure 1
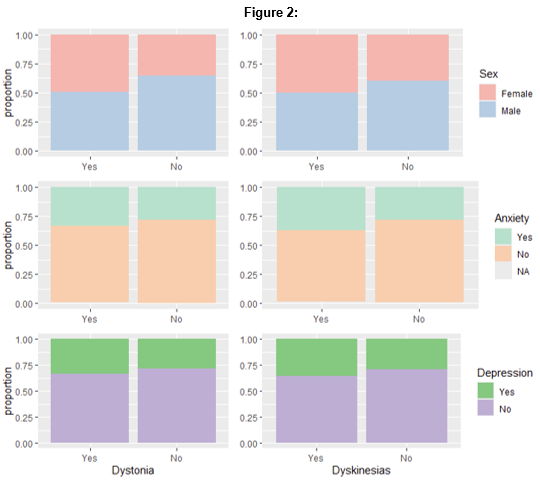
Figure 2
References: 1. Jankovic, J. & Tintner, R. Dystonia and parkinsonism. Parkinsonism Relat Disord 8, 109–121 (2001).
2. Bozi, M. & Bhatia, K. P. Paroxysmal exercise-induced dystonia as a presenting feature of young-onset Parkinson’s disease. Mov Disord 18, 1545–1547 (2003).
3. Stephen, C. D. The Dystonias. Continuum (Minneap Minn) 28, 1435–1475 (2022).
4. Berman, B. D. et al. Psychiatric associations of adult-onset focal dystonia phenotypes. J Neurol Neurosurg Psychiatry 88, 595–602 (2017).
To cite this abstract in AMA style:
L. Xavier, A. Eid, H. Hwang, J. Perlmutter, P. Kotzbauer, M. Campbell, S. Norris. The Unique Clinical Profile of Dystonia in Parkinson Disease [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/the-unique-clinical-profile-of-dystonia-in-parkinson-disease/. Accessed April 6, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/the-unique-clinical-profile-of-dystonia-in-parkinson-disease/