Category: Pediatric Movement Disorders
Objective: To implement a Quality Improvement initiative analyzing referral patterns to an Ontario pediatric movement disorder clinic to develop a better understanding of the acceptance, redirection, and rejection rates of referrals. The aim is to increase referral acceptance rates by 15%.
Background: As the only pediatric movement disorders program in Ontario, increasing demand for evaluation necessitates an efficient triaging system. Evidence suggests that there is a great deal of variety in referral practices amongst providers. This process can be improved given that reviewing referrals is a resource intensive process, and rates of redirection and rejection remain significant.1,2 Providing education regarding referral criteria and clear communication with referring providers can assist in reducing appointment wait times.3
Method: All referrals were received through the electronic medical record system. Incoming referrals were assigned to a Nurse Practitioner (NP) for triage. Each referral was reviewed, assessed and triaged according to reason and urgency. A consensus was reached for each referral between the pediatric neurologist and the NP. Referrals were either accepted, redirected to an appropriate specialty service, or declined with recommendations for alternative pathways.
Results: From February 2024 to December 2024, a total of 151 referrals were received. The primary referral reason was dystonia with 23.84%, followed by tics and Tourette Syndrome (TS) 18.54% [Table 1]. Of the total referrals 64.24% were accepted, 28.48% were redirected, and 7.28% were rejected [Table 2]. The majority of the redirected or rejected referrals originated from family physicians, community pediatricians, and the emergency department [Table 3]. The most common reason for redirection was tics/TS, if they were thought to be better served by psychiatry or a community provider, followed by unspecified referrals [Table 4].
Conclusion: The analysis of referral patterns from February 2024 to December 2024 reveals that a significant majority of referrals were accepted. However, more than one-third of referrals were redirected or rejected. The data suggests that family physicians, community pediatricians, and emergency departments are the primary sources of redirected or rejected referrals. This highlights the need for targeted education and communication strategies to improve referral accuracy from these sources.
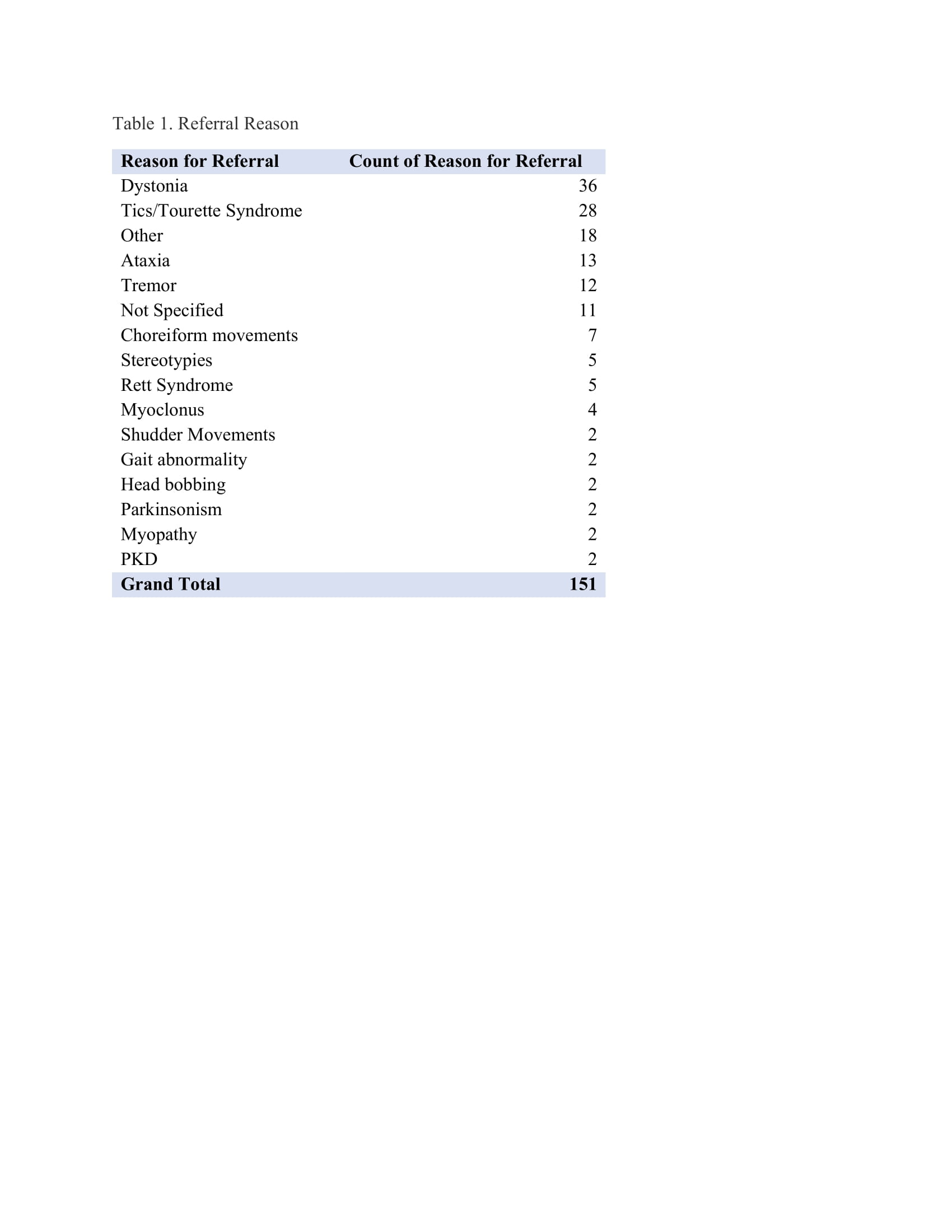
Table 1.
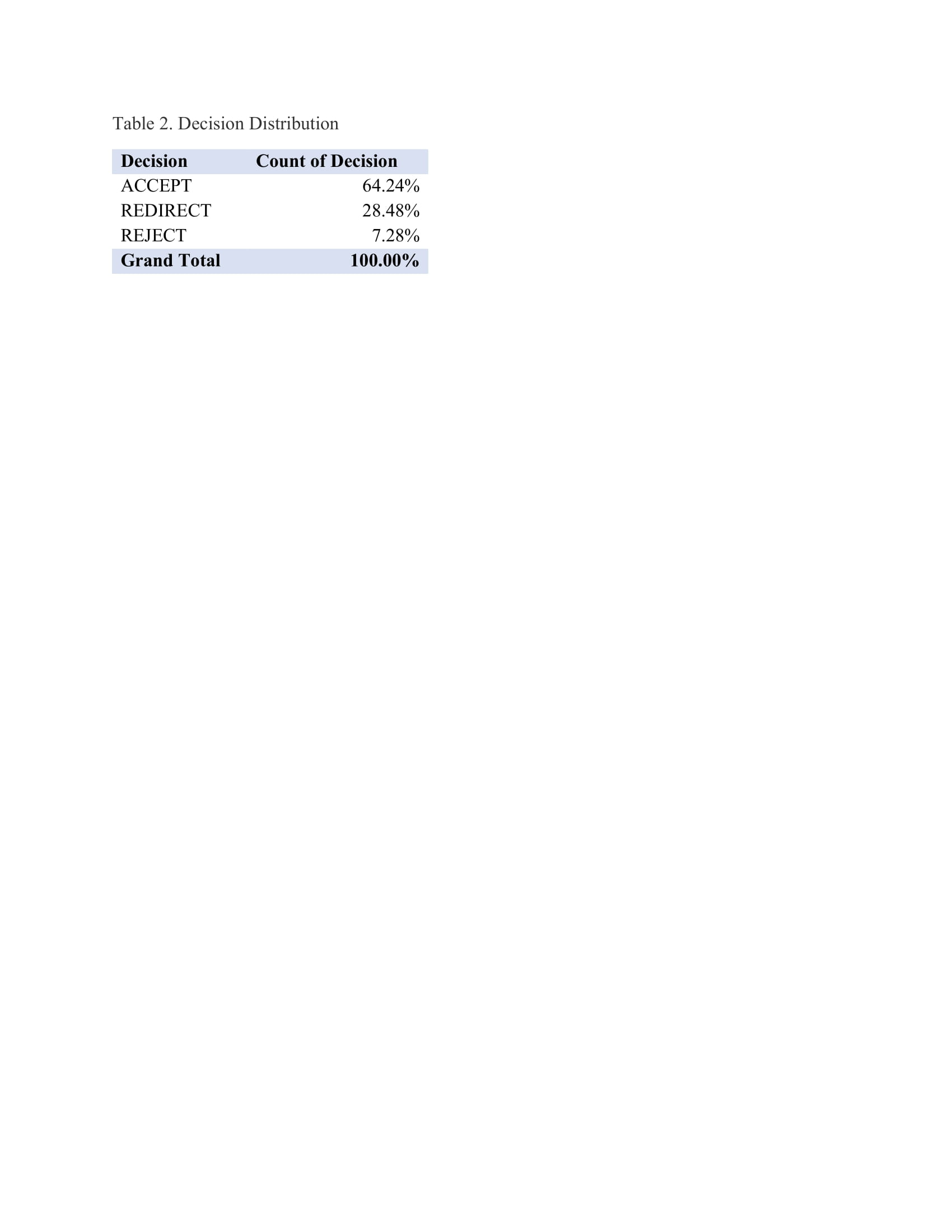
Table 2.
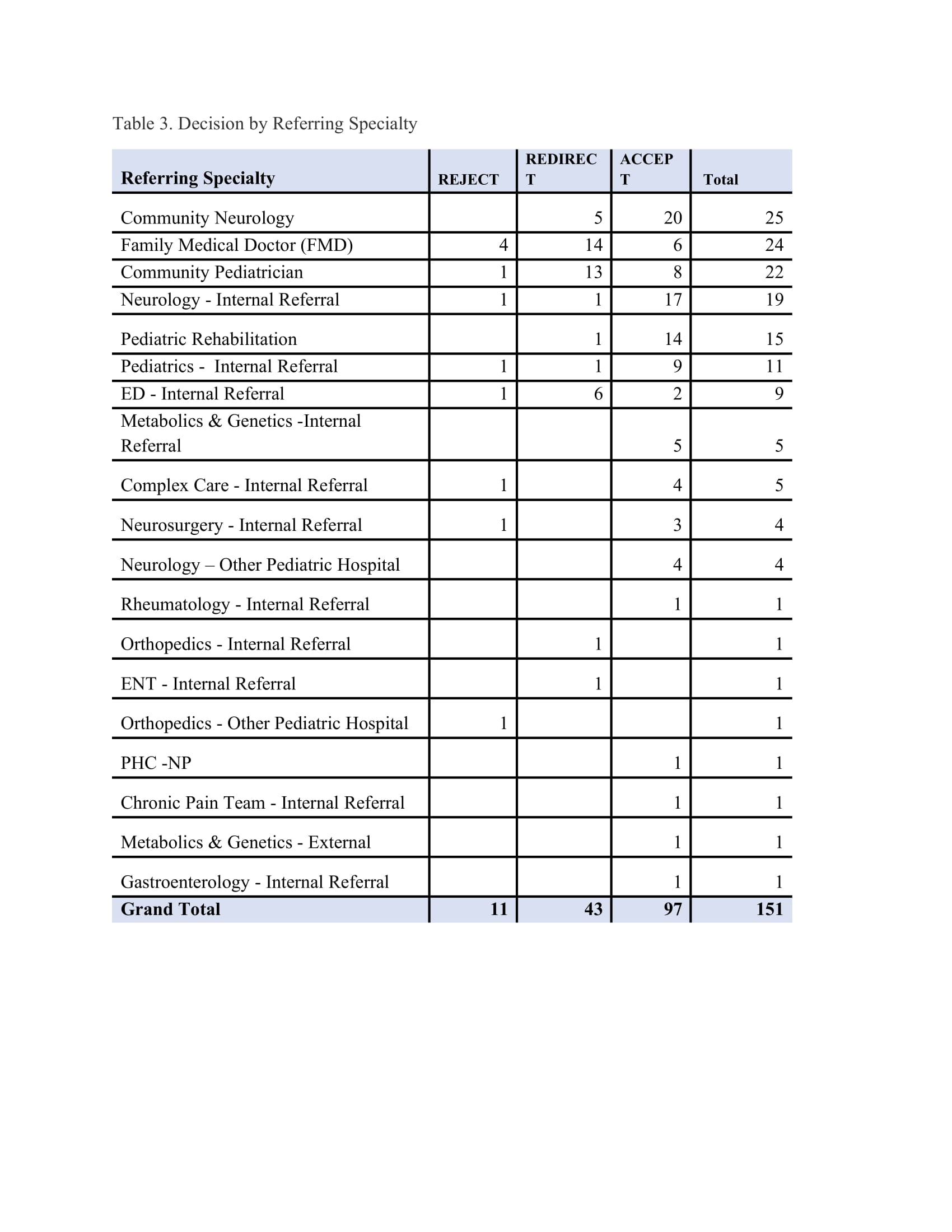
Table 3.
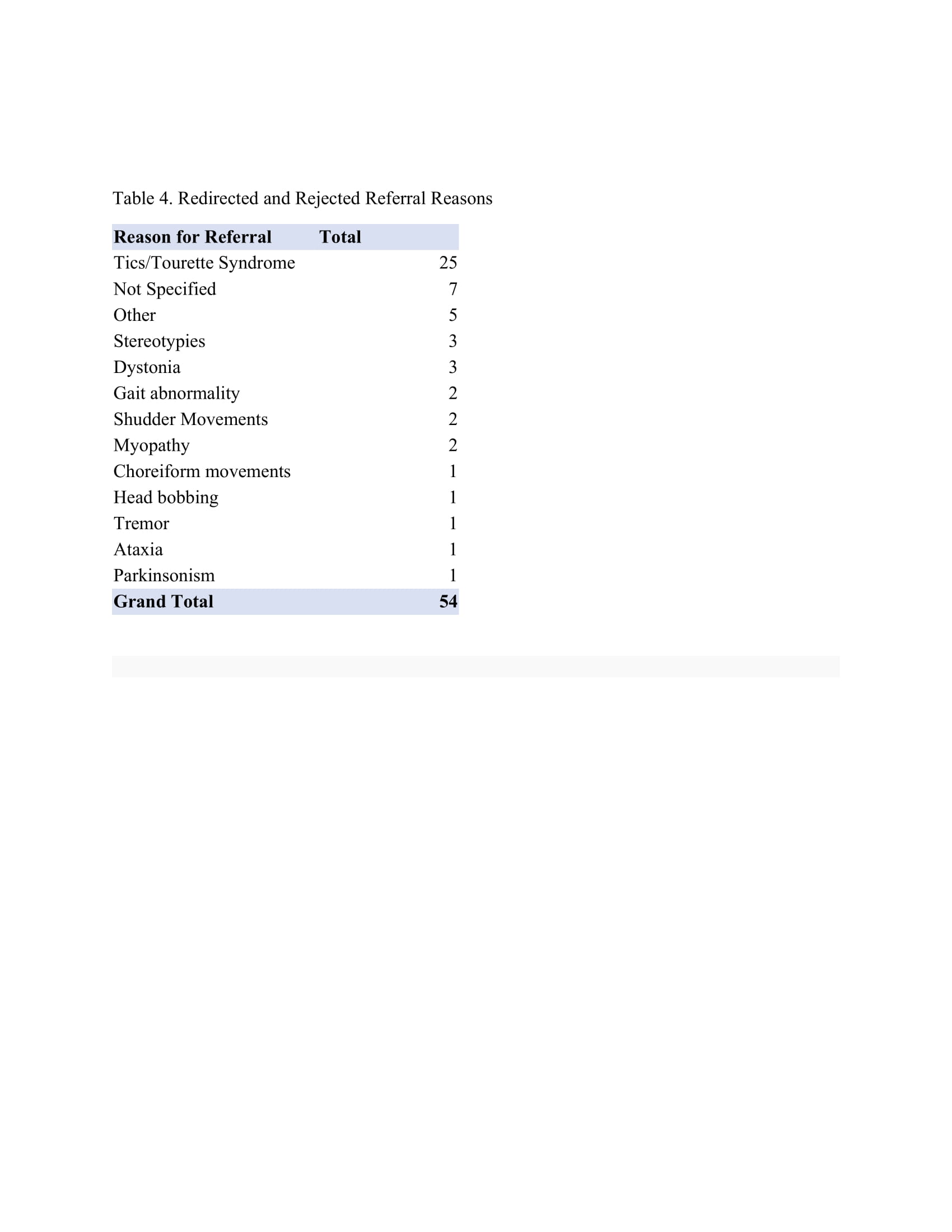
Table 4.
References: 1. Akbari A, Mayhew A, Al-Alawi MA, et al. Interventions to improve outpatient referrals from primary care to secondary care. Cochrane Database Syst Rev. 2008 Oct 8;2008(4):CD005471. doi: 10.1002/14651858.CD005471.pub2
2. MacGregor D, Parker S, MacMillan S, Blais I, Wong E, Robertson CJ, Bruce-Barrett C. Innovation in managing the referral process at a Canadian Pediatric Hospital. Healthc Q. https://pubmed.ncbi.nlm.nih.gov/19553768/
3. Vora SS, Buitrago-Mogollon TL, Mabus SC. A quality improvement approach to ensuring access to specialty care for pediatric patients. Pediatr Qual Saf. 2022;7(3):e566. doi:10.1097/pq9.0000000000000566. PMID: 35720858; PMCID: PMC9197355
To cite this abstract in AMA style:
A. Leblanc-Millar, C. Gorodetsky. Understanding Referral Patterns to a Pediatric Movement Disorders Clinic: A Quality Improvement Project [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/understanding-referral-patterns-to-a-pediatric-movement-disorders-clinic-a-quality-improvement-project/. Accessed April 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/understanding-referral-patterns-to-a-pediatric-movement-disorders-clinic-a-quality-improvement-project/