Session Information
Date: Wednesday, June 22, 2016
Session Title: Ataxiz, Choreas
Session Time: 12:00pm-1:30pm
Objective: To investigate how structural connectivity correlates with the number of CAG repeats, disease evolution and clinical measures in presymptomatic (preHD) and clinical Huntington Disease (HD) patients.
Background: Huntington disease is an autosomal-dominant disease determined by a CAG expansion mutation in the gene encoding the protein huntingtin. Graph theory analysis represents anatomical brain regions as nodes are linked edges, that are the structural connections of white matter tracts (1). We can define a node by its degree of connectivity (nº of edges linked to it), its centrality (nº of shortest paths between any two nodes), its efficiency and its clustering coefficient (probability of forming a group with the neighbouring nodes) (1,2). Mapping these structural networks may help to understand how the neurodegenerative process spreads across structurally interconnected brain regions.
Methods: 84 mutation carriers (31 PreHD and 53 HD patients (stage I-II)) and 76 matched control subjects underwent high-resolution T1-weighted imaging (MDEFT sequence: TR/TE=7.92/2.4ms, FoV=256, voxel-size=1mm3) and Diffusion-weighted imaging (spin-echo EPI sequence: TE/TR=89/8500 ms, voxel size 1.8mm3, 30 isotropically distributed orientations at b=1000 and 6 b=0 images) on a 3T Siemens scanner. Patients were examined by the Unified Huntington’s Disease Rating Scale (UHDRS; Huntington Study Group, 1996). The details of the image processing and network computation can be found in Baggio et al. (2). We used the CAP index (CAP=Age*CAG-33.66) to test the effect of mutation toxicity, corrected by the length of exposure to the mutation toxicity. Pearson correlation test was used.
| Controls (n=76) | PreHD (n=31) | HD (n=53) | X2/t | p-value | |
| Gender (M:F) | 41:35 | 20:11 | 33:20 | 5.63 | NS |
| Age | 44.5 (13.0) | 38.2 (7.2) | 48.1 (13.4) | 5.57 | 0.025 Cnt < PreHD |
| CAG Repeat Length | NA | 42.9 (2.2) | 46.3 (5.8) | -2.95 | 0.004 |
| Disease duration (years) | NA | NA | 7.10 (5.5) | NA | NA |
| TIV | 1408291 (130506.6) | 13933948 (102824.9) | 1321324 (120073.4) | 7.78 | <0.0001 Cnt > HD |
| MMSE | NA | 28 (1.4) | 24.4 (3.9) | 4.06 | <0.0001 |
| UHDRS Motor* | NA | 5.7 (5.3) | 38.4 (14.8) | -10.6 | <0.0001 |
| UHDRS Cognitive | NA | 260.3 (43.2) | 136.6 (46.3) | 10.2 | <0.0001 |
| UHDRS Behavioral* | NA | 7.2 (8) | 18.36 (9.1) | -4.97 | <0.0001 |
| UHDRS Functional | NA | 25 (0) | 17.5 (6) | 6.15 | <0.0001 |
| TFC | NA | 13 (0) | 8.1 (2.6) | 9.42 | <0.0001 |
| Independence scale | NA | 100 (0) | 77.2 (13.4) | 8.34 | <0.0001 |
| Disease burden | NA | 297.9 (65.2) | 454.8 (117.3) | -4.6 | <0.0001 |
Results: All general measures of structural connectivity correlated with the CAP index (p<0.005) 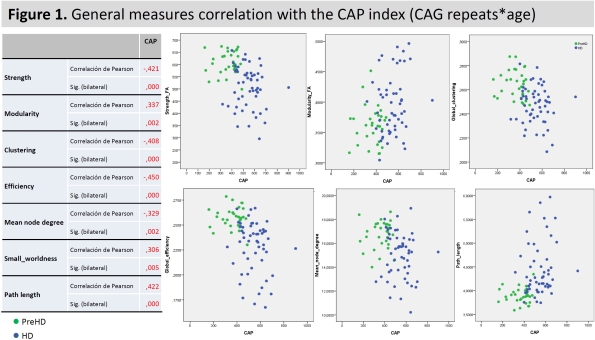 and disease evolution (p<0.008).
and disease evolution (p<0.008).
| Disease Evolution | ||
| Strength | Pearson correlation | -0.445 |
| Sig. (bilateral) | <0.0001 | |
| Modularity | Pearson correlation | 0.298 |
| Sig. (bilateral) | 0.008 | |
| Global clustering | Pearson correlation | -0.460 |
| Sig. (bilateral) | <0.0001 | |
| Global efficiency | Pearson correlation | -0.475 |
| Sig. (bilateral) | <0.0001 | |
| Mean node degree | Pearson correlation | -0.340 |
| Sig. (bilateral) | 0.002 | |
| Small worldness | Pearson correlation | 0.251 |
| Sig. (bilateral) | 0.026 | |
| Path length | Pearson correlation | 0.450 |
| Sig. (bilateral) | <0.0001 |
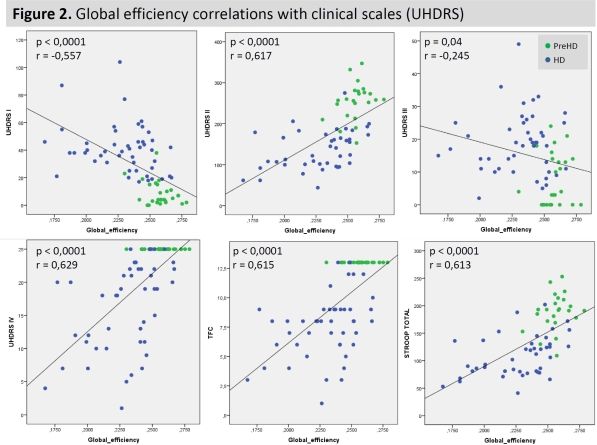
Conclusions: These results provide evidence that the number of CAG repeats together with the time of exposure to the mutation (CAP index) determine the integrity of structural connectivity. Also, structural connectivity measures are correlated with disease evolution. Finally, the efficiency of these connections is related to the clinical scales: the most efficient, the better performance in motor and cognitive scales.
To cite this abstract in AMA style:
C. Sanchez-Castañeda, H. Baggio, U. Sabatini, F. Squitieri, C. Junque. Structural connectivity networks in prodromal and clinical Huntington’s disease [abstract]. Mov Disord. 2016; 31 (suppl 2). https://www.mdsabstracts.org/abstract/structural-connectivity-networks-in-prodromal-and-clinical-huntingtons-disease/. Accessed July 31, 2026.« Back to 2016 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/structural-connectivity-networks-in-prodromal-and-clinical-huntingtons-disease/