Category: Parkinsonism (Other)
Objective: We report a case of secondary parkinsonism due to delayed neurotoxicity induced by ciltacabtagene autoleucel (cilta-cel) chimeric antigen receptor T-cell therapy (CAR-T) as well as the first reported magnetic resonance imaging (MRI) abnormalities.
Background: CAR-T therapy is used to treat relapsed or refractory hematologic malignancies. There has been emerging evidence of delayed neurotoxicity occurring weeks to months following cilta-cel CAR-T therapy. Specifically, in the initial trial of cilta-cel, 6% of patients developed parkinsonism. Delayed cranial neuropathies have also been reported. To date delayed neurotoxicity manifesting as parkinsonism and cranial neuropathy in combination has not been reported. MRI brain in patients with cilta-cel CAR-T related parkinsonism has been reported as normal thus far. Levodopa treatment has been unsuccessful. Limited data suggest treatment with steroid or cyclophosphamide may improve neurotoxicity.
Method: Case Report
Results: A 78-year-old man presented with one month of slowness and abnormal gait after cilta-cel CAR-T therapy (post-infusion day 81) for relapsed multiple myeloma. Right facial weakness was reported post-infusion day 91. Neurologic exam demonstrated prominent hypomimia and bradyphrenia along with asymmetric rigidity, bradykinesia, and a parkinsonian gait. A lower motor neuron pattern right facial nerve palsy was also seen. MRI brain demonstrated bilateral T1 basal ganglia hyperintensity compared to MRI prior to CAR-T therapy [figure1]. Cerebrospinal fluid was without evidence of infection or malignancy. The patient was treated with cyclophosphamide, intravenous immunoglobulin, and methylprednisolone.
Conclusion: This is the first reported case of a patient with both parkinsonism and cranial neuropathy after cilta-cel CAR-T therapy. This is also the first case with abnormal MRI findings of basal ganglia T1 hyperintensity. This case highlights the importance of recognizing parkinsonism as a possible delayed neurotoxicity related to cilta-cel CAR-T. As these symptoms may emerge months after therapy, it is conceivable that this could mimic neurodegenerative parkinsonism. Recognition of atypical features such as cranial neuropathy and abnormal brain MRI may assist in diagnosis. Further investigations are needed examining imaging abnormalities in other cases. Further study is also needed as to treatment approach and outcomes.
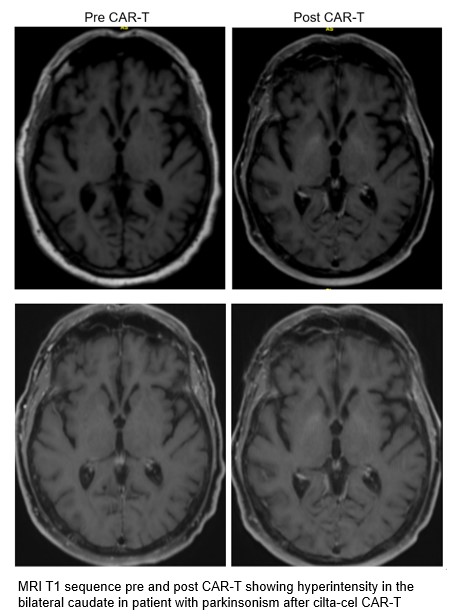
Figure 1
References: 1- Gust J. BCMA-CAR T-cell treatment–associated parkinsonism. Blood. 2023;142(14):1181-1183. doi:https://doi.org/10.1182/blood.2023021860
2- Graham CE, Lee WH, Wiggin HR, et al. Chemotherapy-induced reversal of ciltacabtagene autoleucel–associated movement and neurocognitive toxicity. Blood. 2023;142(14):1248-1252. doi:https://doi.org/10.1182/blood.2023021429
3- Karschnia P, Miller KC, Yee AJ, et al. Neurologic toxicities following adoptive immunotherapy with BCMA-directed CAR T cells. Blood. 2023;142(14):1243-1248. doi:https://doi.org/10.1182/blood.2023020571
To cite this abstract in AMA style:
M. Murzello, A. Pena. Parkinsonism Due to Delayed Neurotoxicity of CAR-T Therapy [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/parkinsonism-due-to-delayed-neurotoxicity-of-car-t-therapy/. Accessed July 7, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/parkinsonism-due-to-delayed-neurotoxicity-of-car-t-therapy/