Category: Rare Neurometabolic Diseases
Objective: To develop a step-by-step diagnostic approach to aceruloplasminemia with initial presentation of movement disorders
Background: Aceruloplasminemia is a rare iron overload disorder with autosomal recessive inheritance. Neurological findings include movement disorders, blepharospasm, grimacing, facial and cervical dystonia, tremors, parkinsonism, chorea and ataxia, gait ataxia, and dysarthria. Cognitive impairment may also be present. Systemic diseases such as diabetes mellitus and anemia. (1)
Method: 64-year-old female patient who presented vertical cervical tremor associated with recent and immediate memory loss in 2019. Over the following year, she presented with limb rigidity, slowness and unsteadiness when walking, retropulsed falls, and dysarthria. On neurological examination, choreic head and limb movements, peripheral facial paralysis, limb rigidity, bradikinesia, ataxic gait, dysrhythmia, gait limitation, unsteady gait or requiring assistance when walking, and preserved involuntary movements. . Mild to moderate multidomain cognitive disorder.
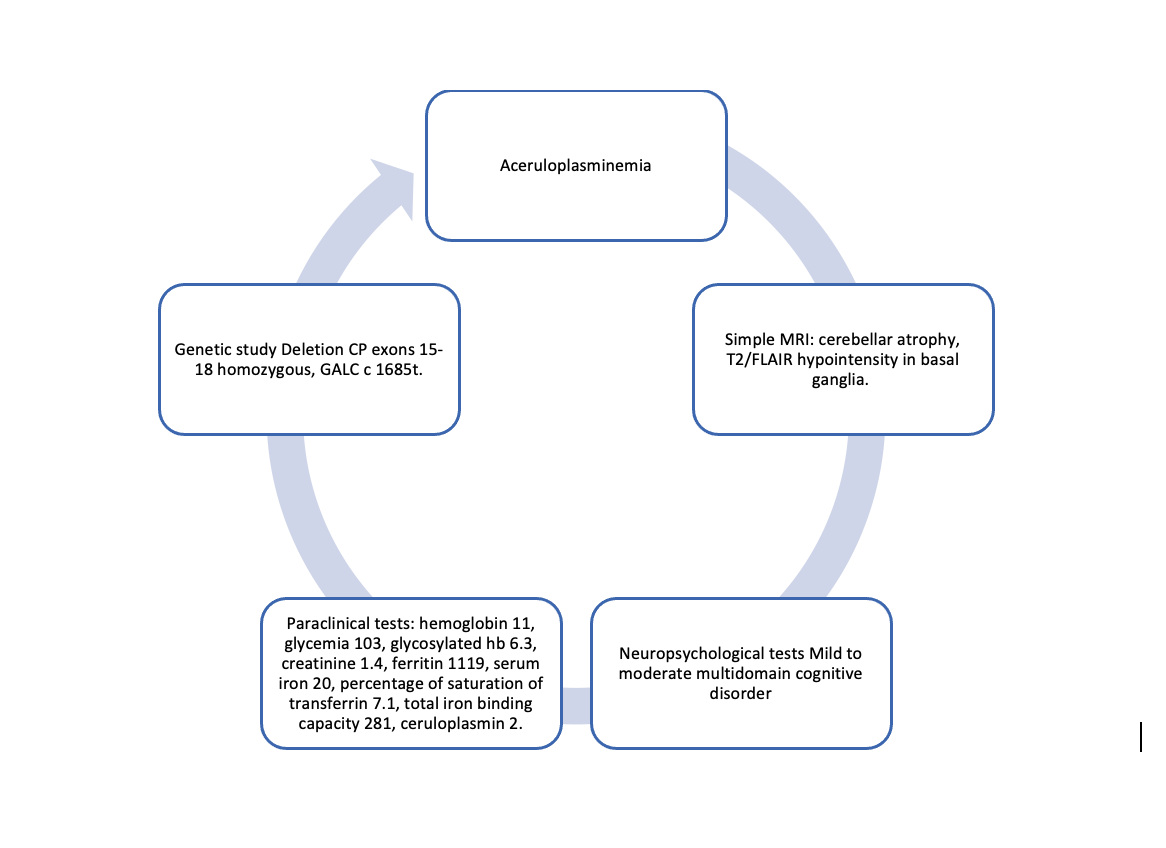
Initially, a diagnosis of atypical parkinsonism with multiple system atrophy was considered, and the patient was treated for several months with levodopa and carbidopa, with no response. Additional studies revealed abnormalities in glucose metabolism, hyperglycemia, and microcytic anemia. A brain MRI was performed, which showed cerebellar atrophy and T2/FLAIR hypointensity in the basal ganglia. Therefore, it was decided to initiate studies on iron metabolism. Elevated ferritin, decreased blood iron levels, and decreased ceruloplasmin levels were found. Finally, a genetic study was also performed with homozygous deletion of CP exons 15-18, GALC c 1685t
Results: Hemoglobin 11, glycemia 103, glycosylated hb 6.3, creatinine 1.4, ferritin 1119, serum iron 20, percentage of saturation of transferrin 7.1, total iron binding capacity 281, ceruloplasmin 2.
Conclusion: Iron metabolism disorders are rare conditions that require a comprehensive approach when patients initially present with movement disorders. This is because not only neurological signs but also associated systemic conditions must be considered. In this case, I presented a patient with progressive movement disorders and cognitive impairment, with glucose metabolism disorders, anemia, elevated ferritin, low ceric iron, decreased ceruloplasmin levels, and a genetic study with homozygous deletion in CP.
Exams
References: 1. Miyajima H, Hosoi Y. Aceruloplasminemia. 2003 Aug 12 [updated 2018 Sep 27]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025.
To cite this abstract in AMA style:
A. Camargo. Movement disorders as a manifestation of aceruloplasminemia a case report [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/movement-disorders-as-a-manifestation-of-aceruloplasminemia-a-case-report/. Accessed July 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/movement-disorders-as-a-manifestation-of-aceruloplasminemia-a-case-report/