Category: Ataxia
Objective: To report a case of CANVAS initially misdiagnosed as subacute labyrinthitis and Meniere’s disease, highlighting the diagnostic challenges and the importance of recognizing this rare syndrome in patients with progressive vestibular and sensory symptoms.
Background: The combination of cerebellar ataxia with axonal sensory neuropathy and bilateral vestibular areflexia is a rare, slowly progressive neurodegenerative disorder. CANVAS often poses diagnostic challenges because of its subtle onset and similarities to other neurodegenerative diseases.
Method: A 58-year-old female presented with a nine-month history of progressive unsteadiness, episodic vertigo, nausea, and sensory disturbances in the lower limbs. Due to her ongoing dizziness and unbalance, she was first diagnosed with labyrinthitis and then Meniere’s illness. Resistance to vestibular suppressants and the lack of variable hearing loss, however, suggested a different diagnosis. A thorough neurological evaluation that included brain MRI, electrophysiological testing, and vestibular function tests was conducted. Genetic testing was recommended to confirm the suspected diagnosis of CANVAS, but the patient declined due to financial constraints.
Results: Cerebellar ataxia, bilateral lower limb sensory loss, absent deep tendon reflexes, and marked bidirectional nystagmus were all found during the neurological test. Bilateral vestibular areflexia was established by video head impulse testing (vHIT). Electroneurography demonstrated sensory neuronopathy, and brain MRI showed mild cerebellar atrophy, particularly in the vermis, without evidence of central demyelination or structural abnormalities suggestive of other neurodegenerative conditions. The diagnosis of CANVAS was highly supported by the combination of clinical, electrophysiological, and imaging evidence, even if genetic confirmation was not feasible due to financial constraints CANVAS.
Conclusion: Suspicion of CANVAS should be raised in the presence of bilateral vestibular impairment, sensory neuropathy, progressive ataxia, and severe bidirectional nystagmus. The diagnosis is further supported by moderate cerebellar atrophy seen on MRI. When genetic testing is not available, a diagnosis can nevertheless be made using clinical and paraclinical findings, even though genetic testing is the gold standard for confirmation. Patient care can be enhanced, and needless treatments can be avoided, by recognizing CANVAS.
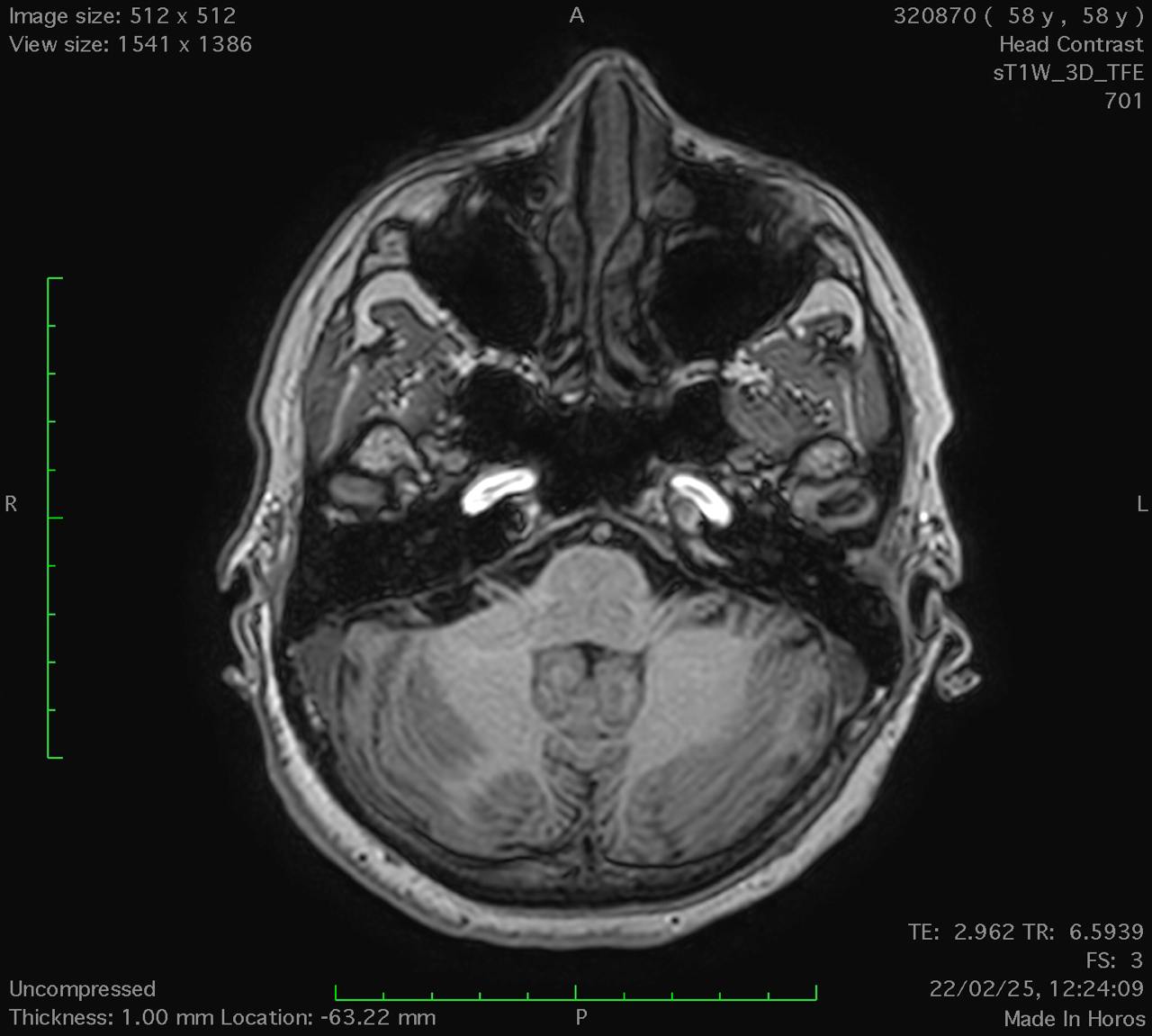
Axial T1-weighted MRI.
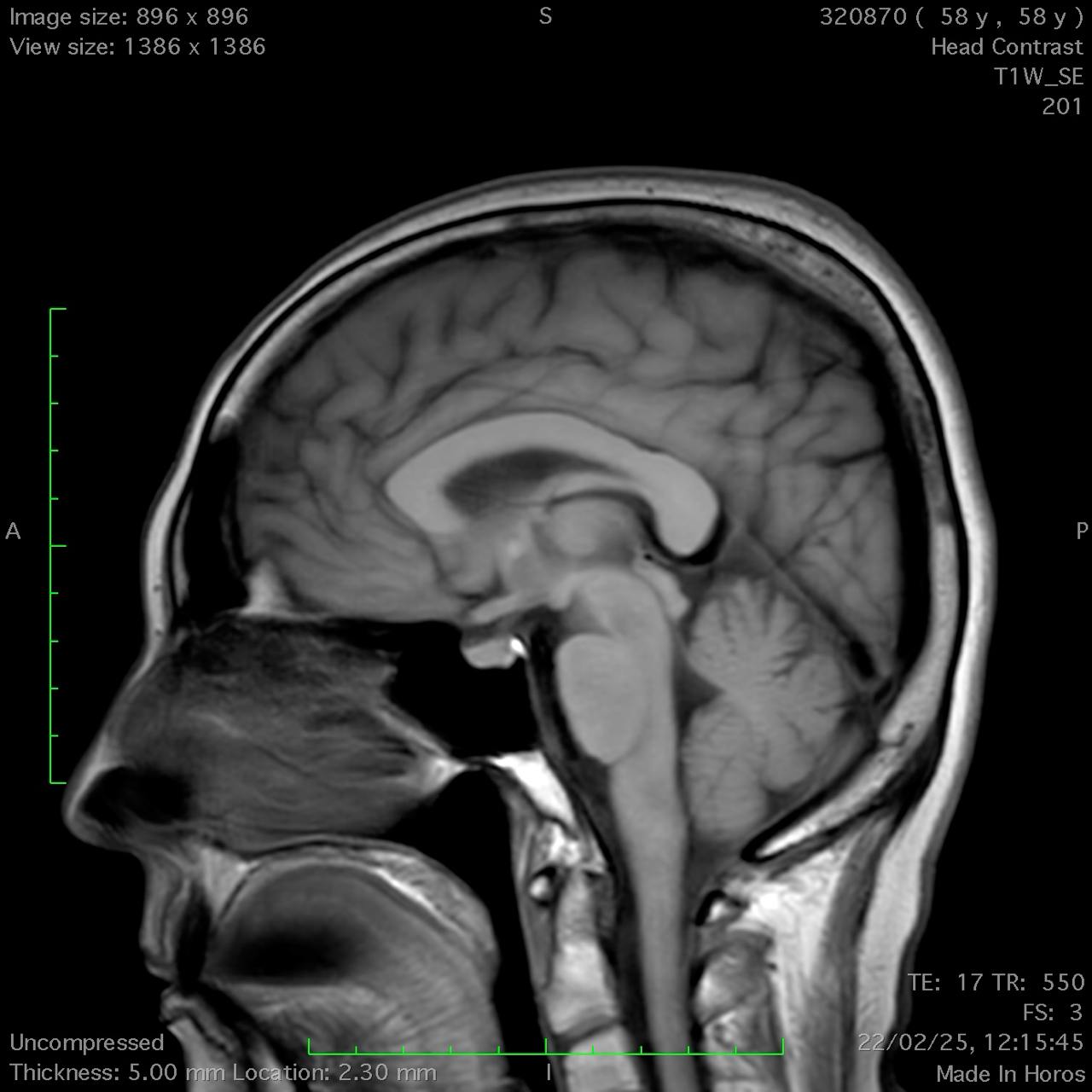
Sagittal T1-weighted MRI.

Sagittal T1-weighted MRI (T1W).
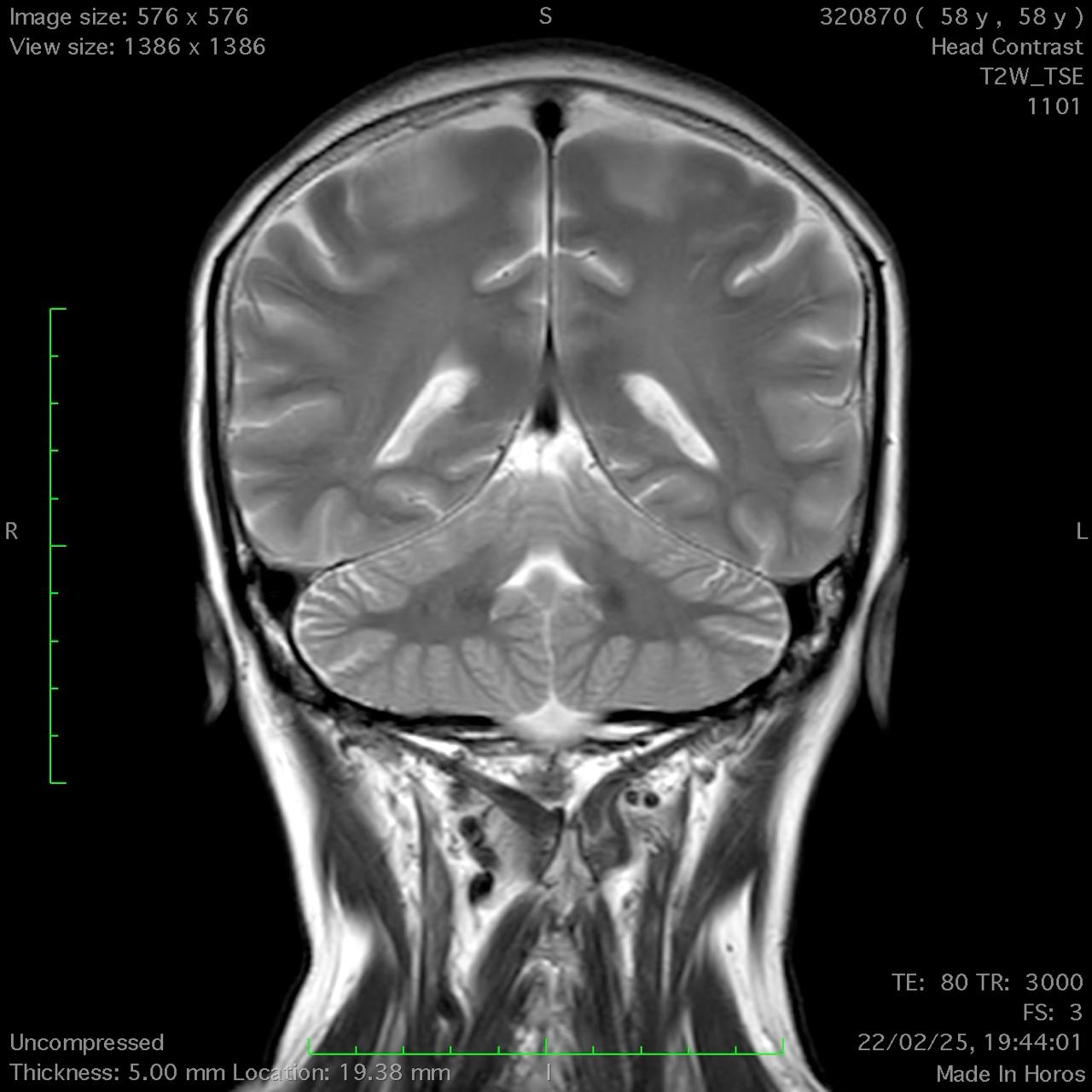
Coronal T2-weighted MRI.
To cite this abstract in AMA style:
Y. Nishonova, B. Mukhammedaminov, N. Aripova, L. Kenjaeva. A Case of CANVAS Misdiagnosed as Subacute Labyrinthitis and Meniere’s Disease [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/a-case-of-canvas-misdiagnosed-as-subacute-labyrinthitis-and-menieres-disease/. Accessed July 7, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/a-case-of-canvas-misdiagnosed-as-subacute-labyrinthitis-and-menieres-disease/