Category: Non-Dystonia (Other)
Objective: To describe hyperkinetic movements consistent with integrated gestural motor behaviors following acute infarction of the insular cortex and parietal lobe.
Background: Involuntary movement disorders occur after 1-4% of strokes, often in infarcts involving the basal ganglia and thalamus and commonly include hemichorea-hemiballism (HCHB), acute dystonia, and tremor. Integrated gestural motor behaviors are complex seizures characterized by naturalistic, semi-purposeful appearing, repetitive movements, and can be difficult to distinguish from other hypermotor phenomenon.
Method: A 69-year-old man presented with sudden left arm sensory loss, asomatagnosia, and weakness. CT-angiogram showed a right MCA-M2 occlusion. He received tenecteplase with rapid symptom improvement. Two hours post-thrombolysis, he exhibited involuntary, hyperkinetic, quasi-purposeful left arm movements seemingly incorporated into voluntary actions including grasping, lasting approximately 30 minutes. MRI revealed an acute infarct in the right posterior insular cortex and parietal lobe [figure 1]. Short-term EEG showed no epileptiform discharges.
Results: The hyperkinetic movements were attributed to insular ictal activity causing integrated gestural motor behaviors, defined as complex hyperkinetic seizures with incorporated identifiable movement sequences such as grasping, tapping, or hitting, following a recognizable but exaggerated pattern. These uncommon movements are typically associated with frontal lobe and insular seizures [1].
Post-stroke HCHB was a differential. Although the stroke spared the traditionally implicated subthalamic nucleus (STN) or basal ganglia, a hyperdirect cortex-STN pathway has been linked to HCHB after frontal and parietal cortical lesions [2]. Reduced cortical input causes STN hypofunction, disinhibiting the thalamus, and leading to direct-indirect pathway imbalance. However, the brief duration and stereotyped repetition made this unlikely.
Holmes tremor was considered given low amplitude, low frequency, and initial wing-beating present at rest and action. However, grasping is unusual as voluntary movements aggravate the tremor, and there was no ischemia in the cerebello-rubral pathway structures.
Conclusion: Gestural motor behaviors are an underrecognized seizure semiology that can mimic other hyperkinetic movements. Subtle differences in the characteristics in conjunction with radiographic localization help ascertain the etiology.
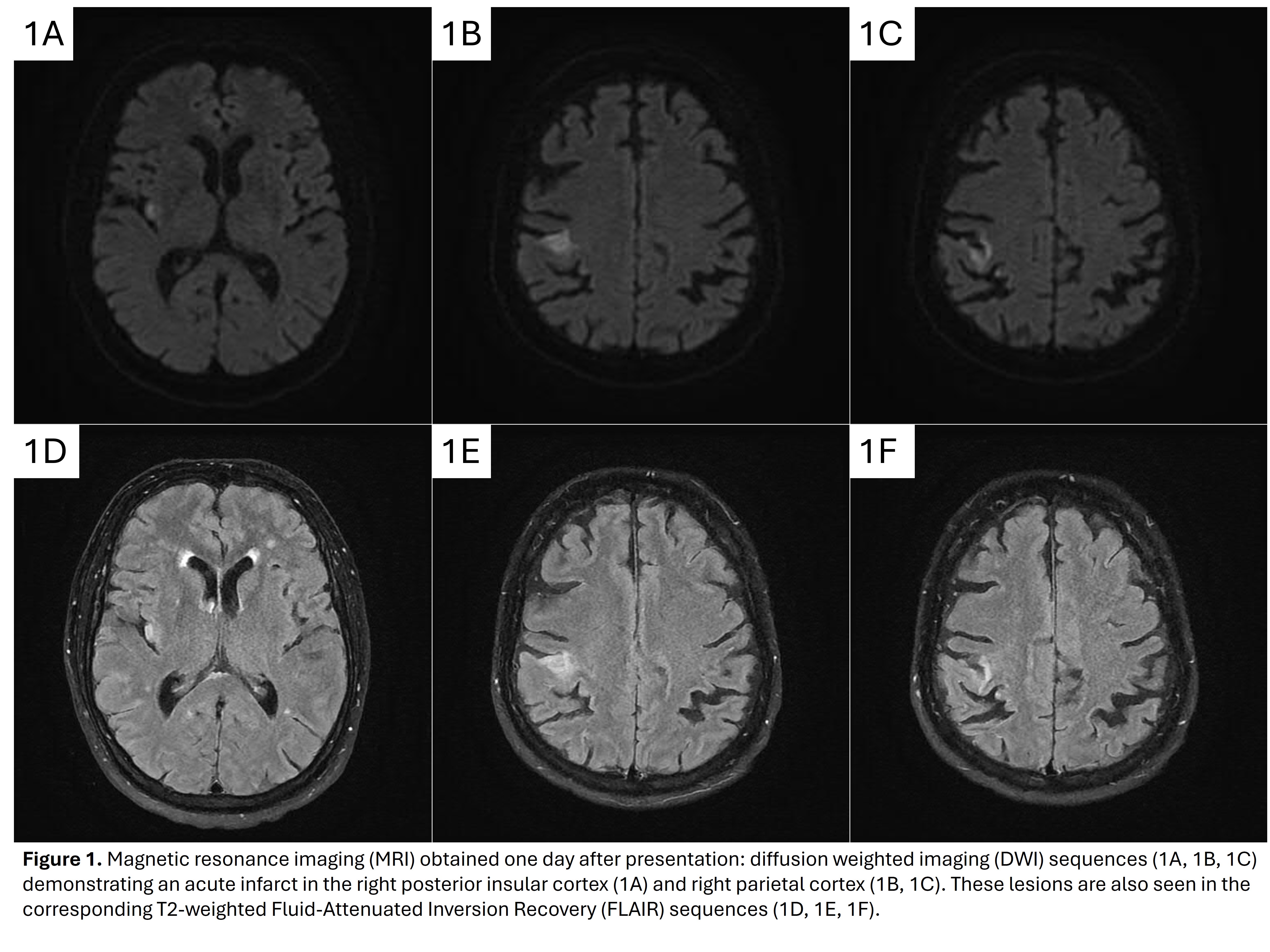
Figure 1
References: 1. Wang H, McGonigal A, Zhang K, et al. Semiologic subgroups of insulo-opercular seizures based on connectional architecture atlas. Epilepsia. 2020;61(5):984-994. doi:10.1111/epi.16501
2. Carbayo Á, Sarto J, Santana D, Compta Y, Urra X. Hemichorea as Presentation of Acute Cortical Ischemic Stroke. Case Series and Review of the Literature. J Stroke Cerebrovasc Dis. 2020;29(10):105150. doi:10.1016/j.jstrokecerebrovasdis.2020.105150
To cite this abstract in AMA style:
T. Modi, T. Zhang, E. Schipani, M. Bates, N. Mccall-Cray, P. Reuter, E. Scharf. Integrated Gestural Motor Behaviors after Insular Infarction: A Case Report [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/integrated-gestural-motor-behaviors-after-insular-infarction-a-case-report/. Accessed July 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/integrated-gestural-motor-behaviors-after-insular-infarction-a-case-report/