Objective: N/A
Background: Runner’s dystonia (RD) is a rare adult-onset focal limb task-specific dystonia. Most predominant phenotype of RD is reported to be dystonic foot equinus. We present a case with an unusual gait abnormality that may be under-recognized.
Method: N/A
Results: Patient is a 48-year-old, right-footed female runner with 5 years of progressive gait impairment. Symptom onset coincided with increased running mileage (110 miles/week) when her left foot would land everted during her runs. Sports medicine performed compartment pressure testing and suggested chronic exertional lateral compartment syndrome. She underwent lateral and empiric anterior compartment release surgery, which was ineffective. Lumbar spine MRI showed bilateral L5-S1 stenosis; EMG indicated left L5 radiculopathy. Patient then underwent laminotomy, which was also ineffective. Thus, paroxysmal exertional dystonia was considered. She received 100 units of botulinum toxin injections to the left fibularis muscles, which caused excessive weakness. A trial of functional electrical stimulation and oral baclofen slightly improved symptoms. She then experienced anterior ankle pain and shoe friction caused a raised bump, suspected to be fibroma. She received monthly steroid injections in this region, which was followed by an extensor hallucis longus rupture requiring tendon repair.
After she returned to baseline, she was evaluated at NIH. Clinical assessment and computerized motion analysis confirmed task-specific RD. Gait analysis revealed left-sided pelvic protraction, knee hyperextension, and most prominently, ankle eversion with an eversion/plantarflexion “whip”. EMG indicated abnormal timing of muscle activation only with running in evertor muscles. She was re-trialed on a lower dose for toxin, targeting fibularis muscles and plantar flexors, which improved her mileage to 50-60 miles per week.
Conclusion: Abnormal gait patterns, delayed diagnostic journey and multiple invasive procedures are commonly seen with RD. This case highlights uncommon biomechanical features, including a repetitive eversion “whip”. Understanding diverse patterns of RD is crucial to guide patient management and avoid unnecessary medical interventions.
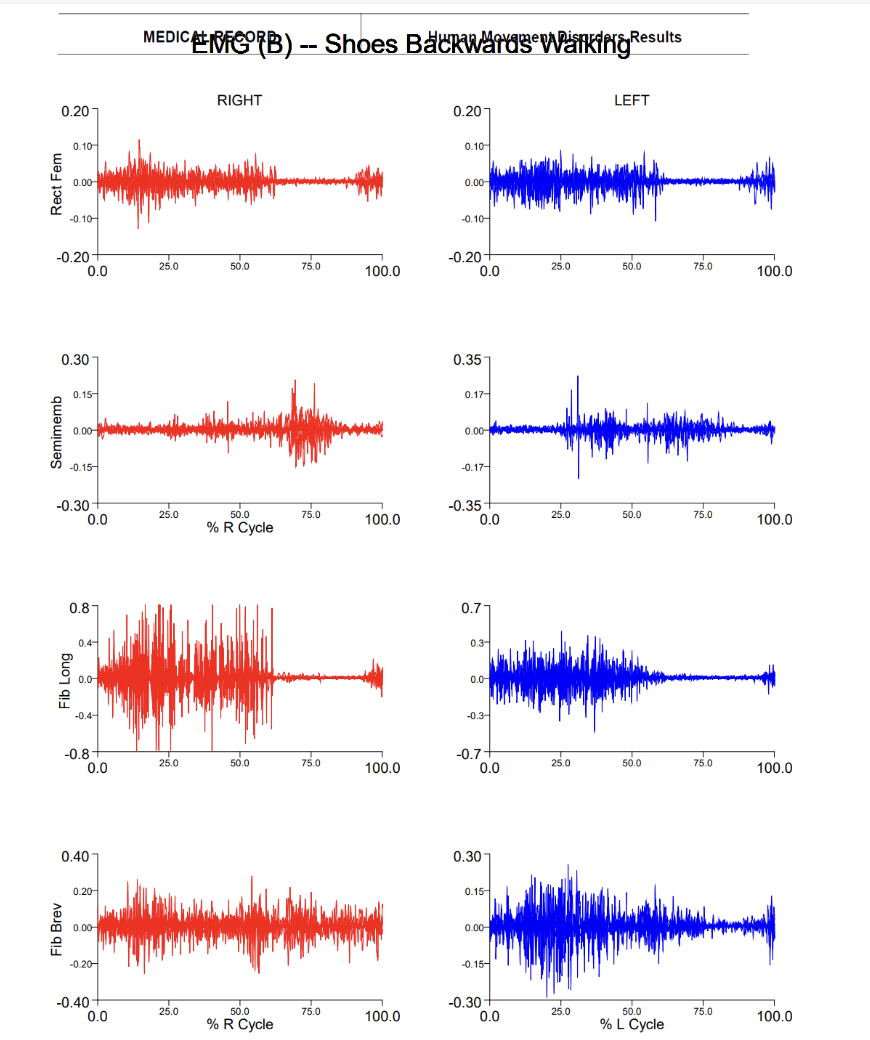
Gait Study: EMG Backward Walking
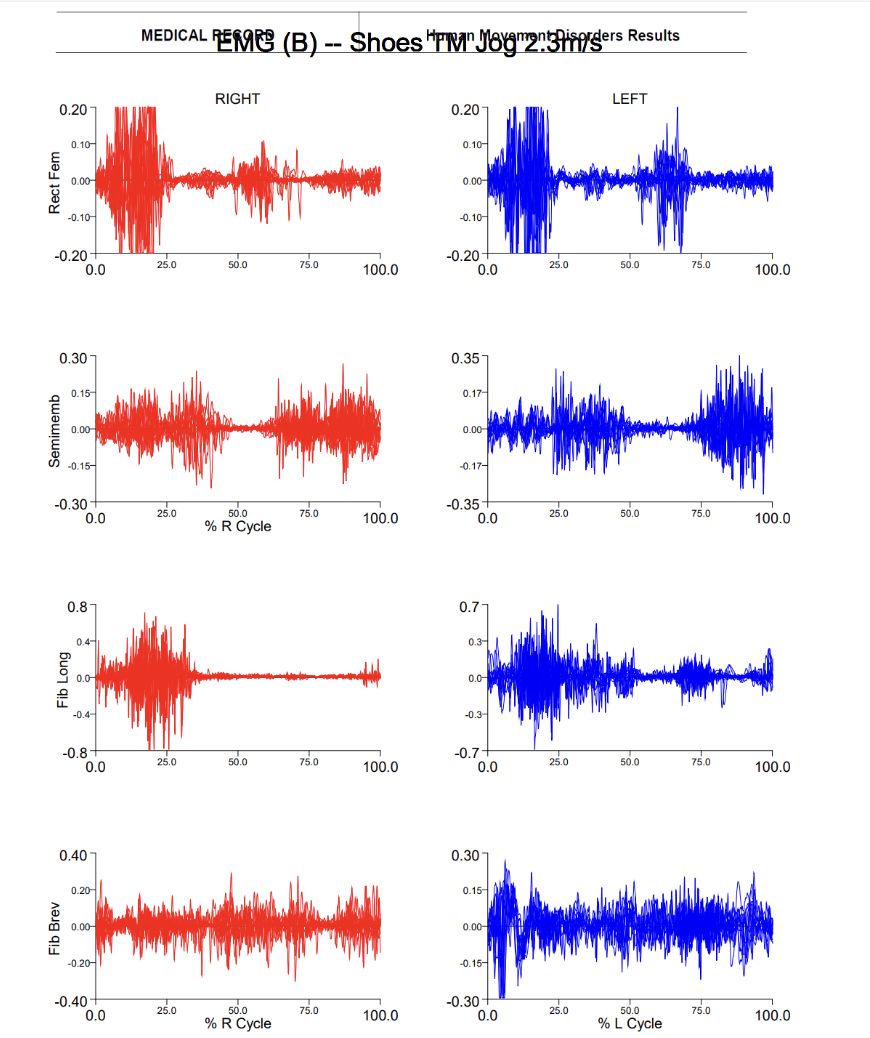
Gait Study: EMG Jogging
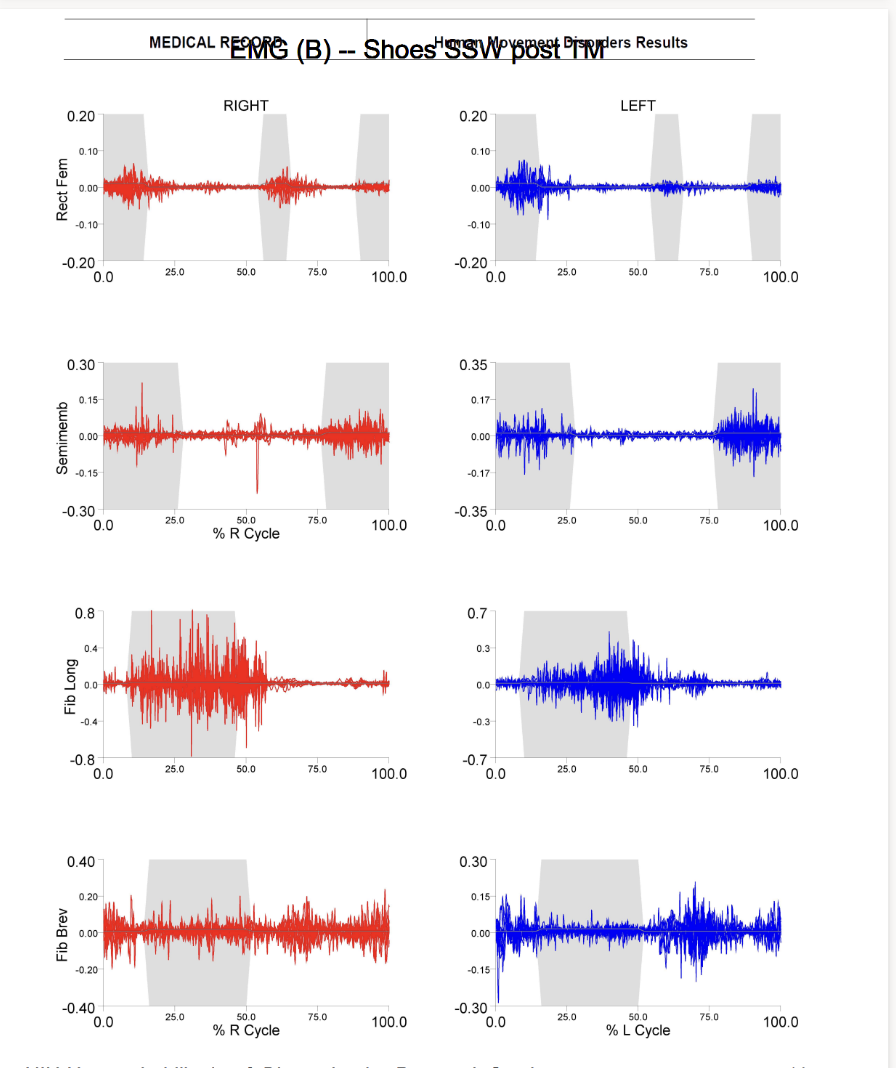
Gait Study: EMG Post-jogging
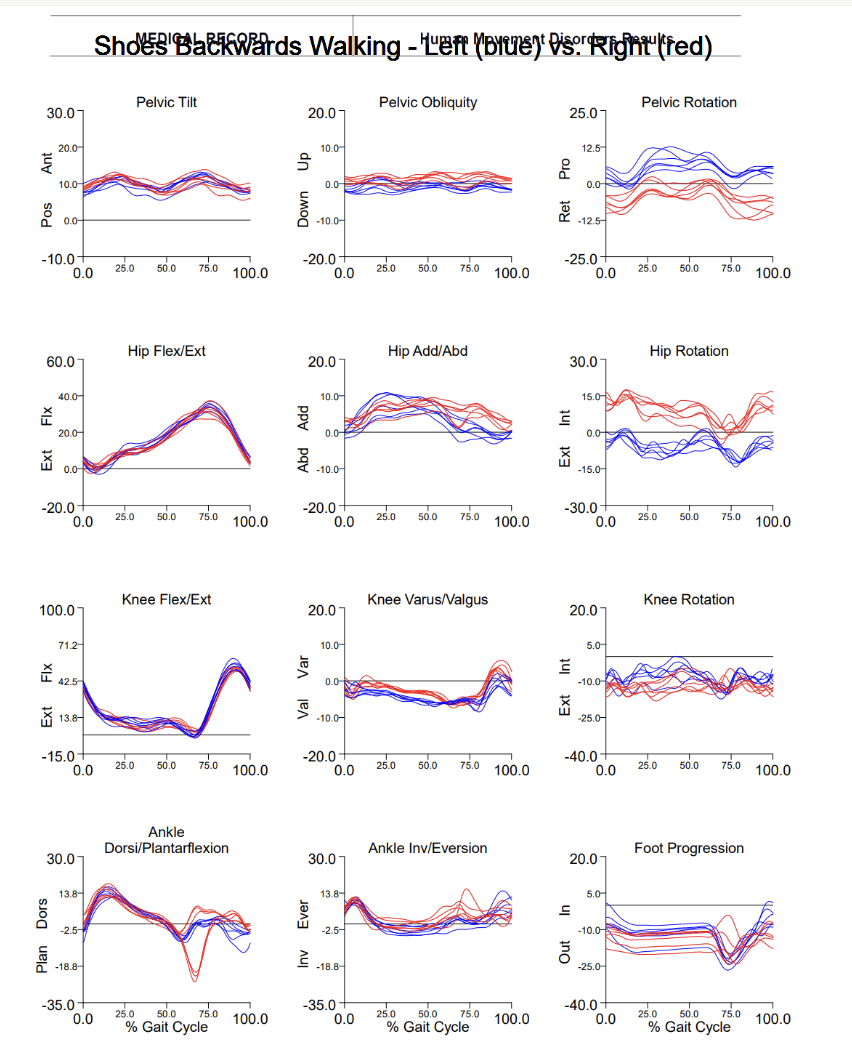
Gait Study: Kinematics Backward Walking
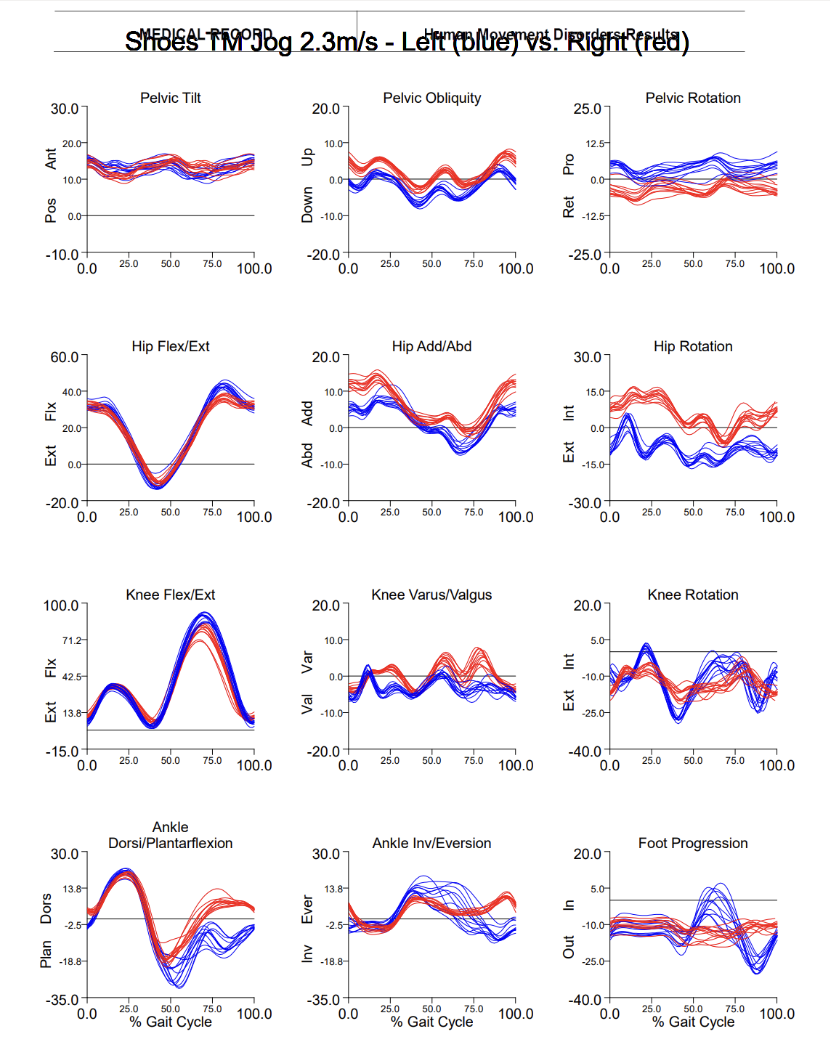
Gait Study: Kinematics Jogging
References: Cutsforth-Gregory, J. K., Ahlskog, J. E., McKeon, A., Burnett, M. S., Matsumoto, J. Y., Hassan, A., & Bower, J. H. (2016). Repetitive exercise dystonia: A difficult to treat hazard of runner and non-runner athletes. Parkinsonism & related disorders, 27, 74–80. https://doi.org/10.1016/j.parkreldis.2016.03.013
Ahmad, O. F., Ghosh, P., Stanley, C., Karp, B., Hallett, M., Lungu, C., & Alter, K. (2018). Electromyographic and Joint Kinematic Patterns in Runner’s Dystonia. Toxins, 10(4), 166. https://doi.org/10.3390/toxins10040166
Ogasawara, I., Hattori, N., Revankar, G. S., Konda, S., Uno, Y., Nakano, T., Kajiyama, Y., Mochizuki, H., & Nakata, K. (2021). Symptom Locus and Symptom Origin Incongruity in Runner’s Dystonia – Case Study of an Elite Female Runner. Frontiers in human neuroscience, 15, 809544. https://doi.org/10.3389/fnhum.2021.809544
To cite this abstract in AMA style:
M. Soliman, A. Mushtaheed, A. Gravunder, J. Matsubara, C. Stanley, C. Zampieri-Gallagher, D. Ehrlich, K. Alter, A. Ly. Case Report: An Atypical Presentation of Runner’s Dystonia [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/case-report-an-atypical-presentation-of-runners-dystonia/. Accessed July 7, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/case-report-an-atypical-presentation-of-runners-dystonia/