Objective: Evaluate dystonia patients with different subtypes using a standardized neurophysiological test battery.
Background: Dystonia pathophysiology is characterized by circuit dysfunction involving the thalamus, basal ganglia, cerebellum, brainstem, spinal cord, and cerebral cortex(1). It is hypothesized that aberrant plastic changes in sensory and motor regions, along with reduced inhibition, result in abnormally increased excitatory tone(2). However, the specific alterations in these circuits are not well understood and may differ across subtypes(3).
Method: We tested 11 patients with cervical dystonia (age 67 10 years; mean standard deviation; 8 women), 5 with blepharospasm (64 11 years; 3 women), 4 with writer’s cramp (64 4 years; 3 women) and 14 age-matched healthy subjects (47 20 years; 5 women). Patients received botulinum toxin injections at least 3 months before the study. We assessed spatial discrimination using JVP domes, temporal discrimination through electrical stimulation of the index finger, spinal cord excitability via cutaneous silent period (CuSP), brainstem excitability through blink reflex recovery curve, motor cortical and cerebellar excitability using paired transcranial magnetic stimulation (TMS).
Results: The comparison of the measurements between groups using Kruskal-Wallis is summarized in Figure 1. Only the CuSP showed significant difference between groups, with writer’s cramp patients showing longer duration and end latency compared to the other groups. Spatial and temporal discrimination tended to be higher in writer’s cramp and lower in blepharospasm and cervical dystonia compared to controls. TMS measures indicated a trend of reduced inhibition and higher excitation in motor cortex and reduced cerebellar inhibition in blepharospasm patients compared with the other groups.
Conclusion: Writer’s cramp dystonia exhibited increased spinal cord inhibition. Additionally, there was a trend toward increased spatial/temporal sensory discrimination thresholds in writer’s cramp, reduced thresholds in cervical dystonia, and reduced sensory discrimination threshold with diminished inhibition in the motor cortex and cerebellum in blepharospasm. These findings suggest that each dystonia subtype may exhibit unique neurophysiological alterations. However, these results are preliminary. Ongoing data collection will help identify the optimal combination of tests to differentiate between subtypes.
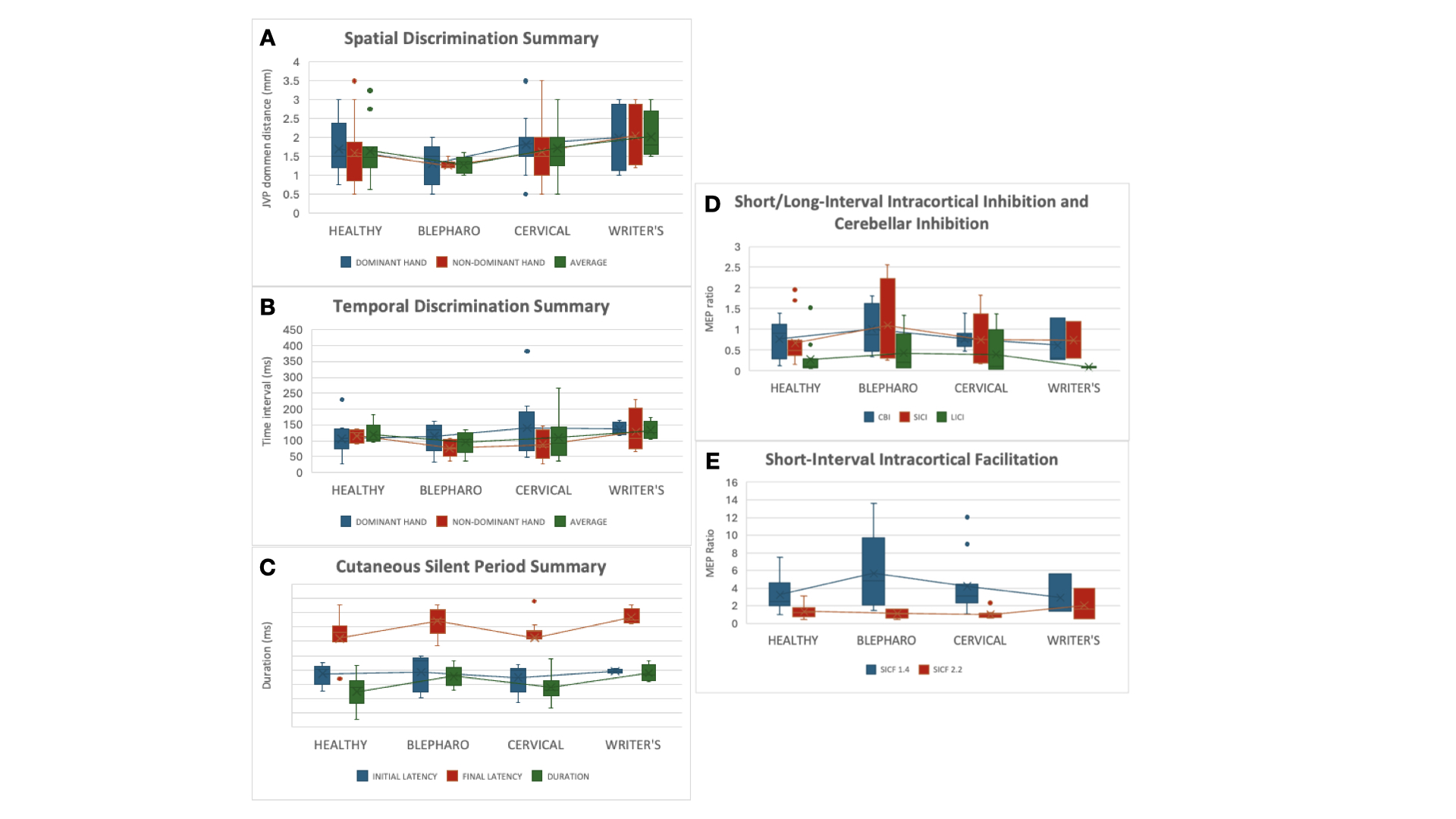
Figure 1
References: 1. Udupa K, Chen R. Motor cortical circuits in Parkinson disease and dystonia. In: Handbook of Clinical Neurology [Internet]. Elsevier; 2019 [cited 2023 Jan 28]. p. 167–86.
2. Latorre A, Rocchi L, Bhatia KP. Delineating the electrophysiological signature of dystonia. Exp Brain Res. 2020 Aug;238(7–8):1685–92.
3. Conte A, Rocchi L, Latorre A, Belvisi D, Rothwell JC, Berardelli A. Ten-Year Reflections on the Neurophysiological Abnormalities of Focal Dystonias in Humans. Mov Disord. 2019 Nov;34(11):1616–28.
To cite this abstract in AMA style:
T. Grippe, N. Sheth, A. Bhattacharya, JC. Chen, N. Raies, H. Taskin, N. Naeini, R. Annirood, JF. Nankoo, J. Baarbe, R. Chen. Multimodal Neurophysiological Evaluation in Patients with Different Dystonia Subtypes [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/multimodal-neurophysiological-evaluation-in-patients-with-different-dystonia-subtypes/. Accessed July 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/multimodal-neurophysiological-evaluation-in-patients-with-different-dystonia-subtypes/