Objective: To describe a case of DBS-responsive laryngeal dystonia in the setting of myoclonus-dystonia secondary to e-sarcoglycan (SGCE) mutation.
Background: DBS is emerging as a promising therapy for laryngeal dystonia [1]. There is evidence of abnormal functional connectivity within the basal ganglia-thalamo-cerebellar pathway, frontoparietal and sensorimotor networks in laryngeal dystonia[2, 3]. Imbalance in dopaminergic transmission, leads to favouring of the direct basal ganglia pathway resulting in dystonia, which GPi-DBS may therapeutically modulate[4]. While, SGCE is DBS-responsive[5], this is the first case of improvement of severe laryngeal dystonia in the condition.
Method: We report on SGCE-related laryngeal dystonia responsive to GPi-DBS
Results: At 12 years, our patient developed began to have gradually worsening speech changes. At 21 years, she developed involuntary upper limb posturing and jerking. There is no family history, including five unaffected siblings. MRI Brain was normal. In addition to typical features of SGCE-related myoclonus dystonia affecting the limbs and trunk, she had a speech pattern suggestive of adductor laryngeal dystonia, including staccato phonation breaks [Table 1]. Nasendoscopy confirmed adductor dystonia with occasional fast contractions, suggestive of myoclonus, and some supraglottic laryngeal constriction. She carried a frameshift variant in SGCE predicted to cause a premature stop codon (NM_003919.3): c.[786_789dup];[=] p.[(Thr264Serfs*7)];[=]. Zonisamide 150mg/day was not tolerated due to neuropsychiatric symptoms. Trihexyphenidyl 1mg daily and levodopa-benserazide 100mg TDS provided little benefit. OnabotulinumtoxinA was given into bilateral thyroarytenoid and right arm muscles every 3 months, with some improvement.
She underwent bilateral GPi-DBS at 25 years. At 2-month follow-up there was marked improvement in limb myoclonus and dystonia. All voice outcome measures improved markedly [Table 1].
Conclusion: GPi-DBS may be beneficial for laryngeal dystonia with SGCE-mutations, in both objective and subjective voice outcomes.
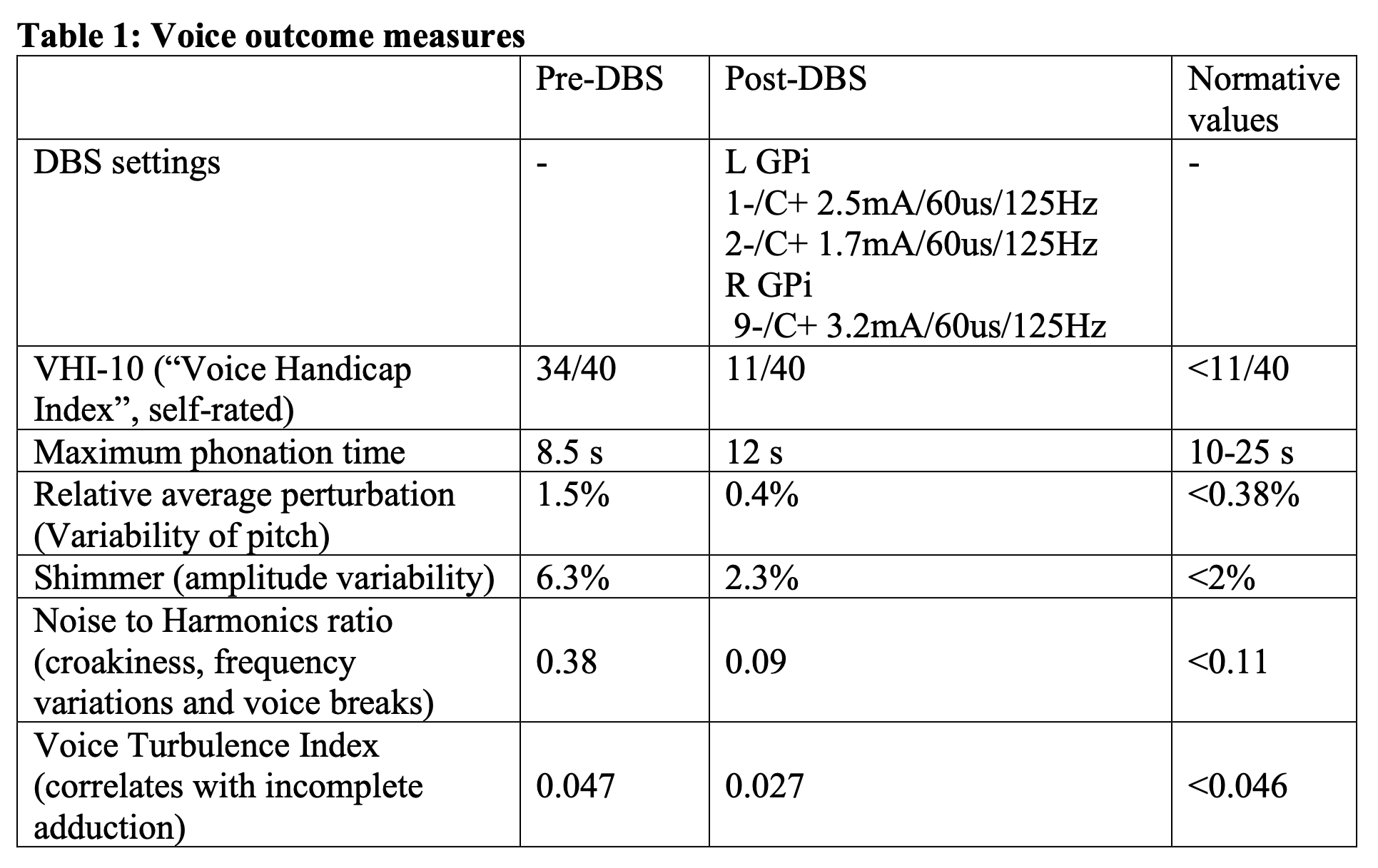
Table 1
References: 1. Evidente VGH, Ponce FA, Evidente MH, Lambert M, Garrett R, Sugumaran M, et al. Adductor Spasmodic Dysphonia Improves with Bilateral Thalamic Deep Brain Stimulation: Report of 3 Cases Done Asleep and Review of Literature. Tremor Other Hyperkinet Mov (N Y). 2020;10:60.
2. Blitzer A, Brin MF, Simonyan K, Ozelius LJ, Frucht SJ. Phenomenology, genetics, and CNS network abnormalities in laryngeal dystonia: A 30-year experience. The Laryngoscope. 2018;128(S1):S1-S9.
3. Simonyan K, Barkmeier-Kraemer J, Blitzer A, Hallett M, Houde JF, Jacobson Kimberley T, et al. Laryngeal Dystonia. Neurology. 2021;96(21):989-1001.
4. Simonyan K, Cho H, Hamzehei Sichani A, Rubien-Thomas E, Hallett M. The direct basal ganglia pathway is hyperfunctional in focal dystonia. Brain. 2017;140(12):3179-90.
5. Azoulay-Zyss J, Roze E, Welter M-L, Navarro S, Yelnik J, Clot F, et al. Bilateral Deep Brain Stimulation of the Pallidum for Myoclonus-Dystonia Due to ε-Sarcoglycan Mutations: A Pilot Study. Archives of Neurology. 2011;68(1):94-8.
To cite this abstract in AMA style:
S. Nagaratnam, D. Wilson, L. Williams, S. Xi, L. Natsis, J. Mcmaster, N. Mahant. GPi-DBS responsive laryngeal dystonia in SGCE myoclonus-dystonia [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/gpi-dbs-responsive-laryngeal-dystonia-in-sgce-myoclonus-dystonia/. Accessed July 7, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/gpi-dbs-responsive-laryngeal-dystonia-in-sgce-myoclonus-dystonia/