Category: Parkinson’s Disease: Clinical Trials
Objective: To evaluate the effectiveness and safety of remote vs. on-site DBS programming in Parkinson’s disease patients with STN-DBS.
Background: Deep brain stimulation (DBS) is the treatment of choice for advanced Parkinson’s disease (PD), with effective postoperative programming being essential for optimal patient outcomes. Telemedicine has expanded access to specialist care, particularly for patients in remote locations or with severe disability.
Method: We conducted a controlled, randomized, prospective, multicenter study at six German university hospitals, enrolling 50 patients with PD who had undergone subthalamic nucleus (STN) DBS. Participants were randomly assigned (1:1) to receive DBS programming either on-site or remotely via the Abbott NeuroSphere™ Virtual Clinic for 90 days post-implantation. The primary endpoint, assessed for non-inferiority, was the UPDRS-III score in the Med On condition at 3 months. Secondary endpoints included UPDRS-I, -II, and -IV, PDQ-39, BDI, MoCA, and the Suicide Ideation Scale.
Results: Patients were randomly assigned to standard-of-care (SoC) on-site or remote DBS programming. The mean age was 64.9 ± 1.54 years for the SoC group and 59.34 ± 2.02 years for the remote group (p = 0.0303). The baseline UPDRS-III score in the Med Off condition was 39.24 ± 2.84 for the SoC group (n = 25) and 33.34 ± 3.30 for the remote group (n = 22) (p = 0.3387). At 90 days, both groups showed a significant reduction in UPDRS-III scores: 14.76 ± 1.79 for the SoC group and 11.82 ± 1.55 for the remote group (p= 0.8363; 95% CI, -7.85 to 1.98; difference in means, -2.93). At the same time, the levodopa-equivalent dose (LEED) decreased similarly in both groups, from 1032.6 ± 101.53 mg/day (SoC) and 944.0 ± 3.30 mg/day (remote) to 457.5 ± 59.80 mg/day (SoC) and 528.7 ± 92.6 mg/day (remote) (p = 0.863). Three patients in the remote arm were excluded due to unsatisfactory improvement with remote programming, one of whom required revision surgery due to incorrect electrode placement.
Conclusion: Remote DBS programming demonstrated non-inferior improvement in PD motor symptoms at 90 days compared to SoC programming. This study provides Class A evidence supporting the efficacy and safety of remote DBS programming for STN-DBS in PD. However, some patients may require in-person optimization for complex symptom management. The trial is registered at ClinicalTrials.gov (NCT05193825).
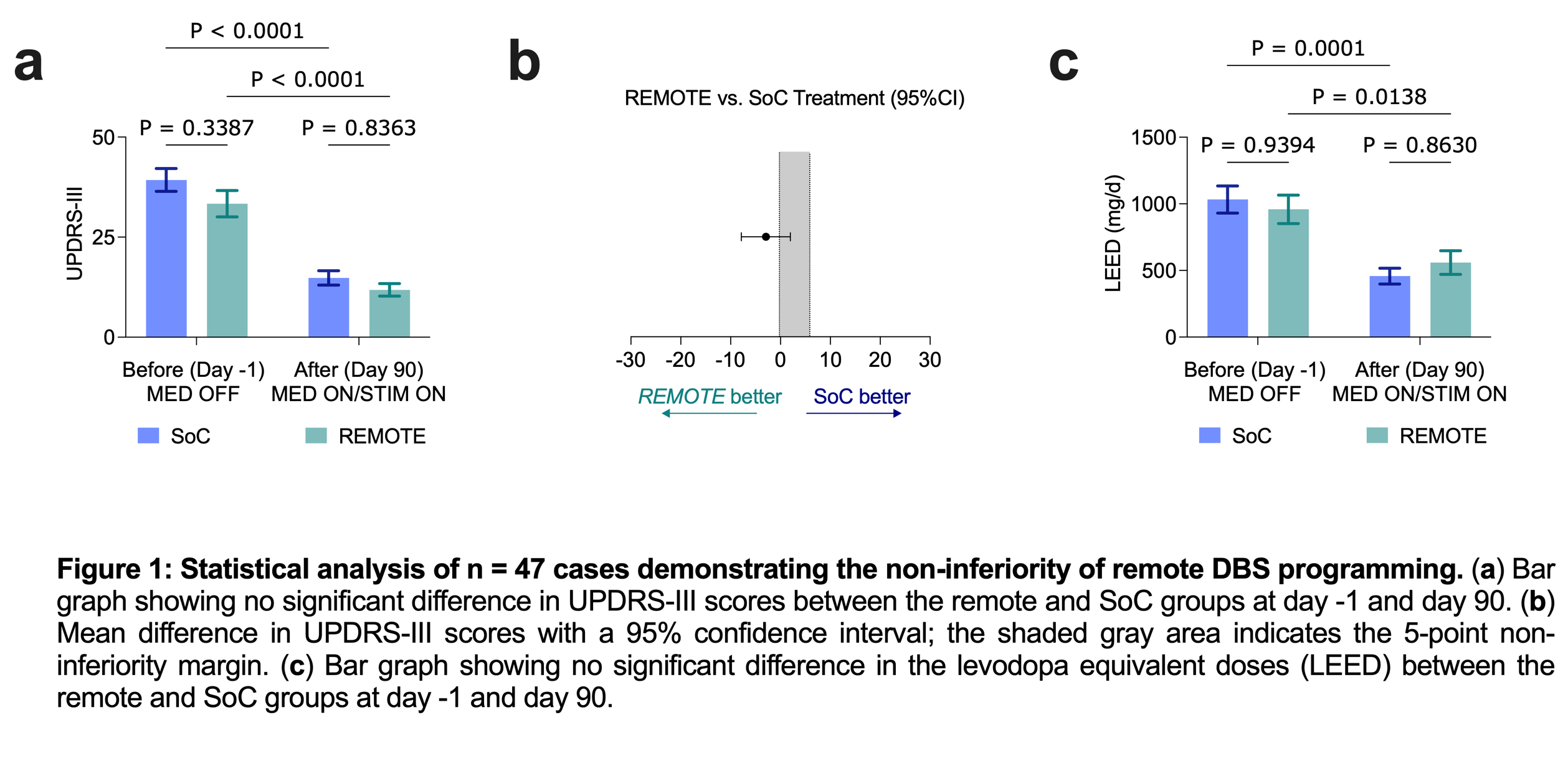
Figure 1
To cite this abstract in AMA style:
J. Shaik, V. Zentsch, C. Buhmann, T. Kinfe, M. Regensburger, J. Rumpf, A. Schnitzler, G. Höglinger, J. Mehrkens, T. Koeglsperger. Remote Deep Brain Stimulation Programming for Parkinson’s Disease: A Multicenter Randomized Non-Inferiority Trial [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/remote-deep-brain-stimulation-programming-for-parkinsons-disease-a-multicenter-randomized-non-inferiority-trial/. Accessed July 5, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/remote-deep-brain-stimulation-programming-for-parkinsons-disease-a-multicenter-randomized-non-inferiority-trial/