Category: Parkinson's Disease: Surgical Therapy
Objective: To share 3 cases presented with seizure and encephalopathy after bilateral subthalamic nucleus deep brain stimulation surgery for Parkinson’s disease that requires removal of the implant.
Background: Peri-lead oedema following STN DBS implantation for PD is increasingly recognised, and seizures are a common presentation. Most cases recovered fully by anti-seizure treatment, steroids and dehydration. However, not every case responds to this treatment.
Method: Case series
Results: The age at presentation was 62, 63 and 74 years old for case 1, 2 and 3. All the patients were female. The duration of Parkinson’s disease prior to surgery was 14 years, 15 years and 8 years respectively. All patients developed symptoms (confusion, disorientation and seizure) after 24 hours post-operation. There was no fever. Investigations performed did not support infections. EEG performed on all the cases showed asymmetric rhythmic slowing with embedded sharp waves with evolution over anterior head region. The MRI brain imaging detected bilateral asymmetrical peri-lead oedema. Despite treatment with anti-seizure and corticosteroid, patients remain encephalopathic. After clinical consideration, decision was made to remove the DBS implants at day 63, 4 and 9 post-operatives respectively. Brain biopsy results from case 2 revealed features consistent with mild acute encephalitis, however, in case 3; it showed ischaemic, reactive changes with no specific inflammatory process. CSF PCR from case 2 indicated Lactococcus lactis 16s rDNA detected, therefore, she received a 4 weeks course of antibiotics. Investigations for porphyria was performed in view of strong family history however; the result was negative. Follow up EEG showed resolution of epileptiform activity. All patients improved soon after and underwent rehabilitation.
Conclusion: Our experiences show that our patients did not improve with conservative treatment. Following DBS implantation, tissue damage is inevitable, initiating neuroinflammatory responses that are integral to the natural wound healing process which manifested as peri-lead oedema and usually self-limiting (1,2). However, we are unsure why our cases had severe idiosyncratic reactions that persisted. As the implant caused patients’ deterioration, removal of implants necessitated it.
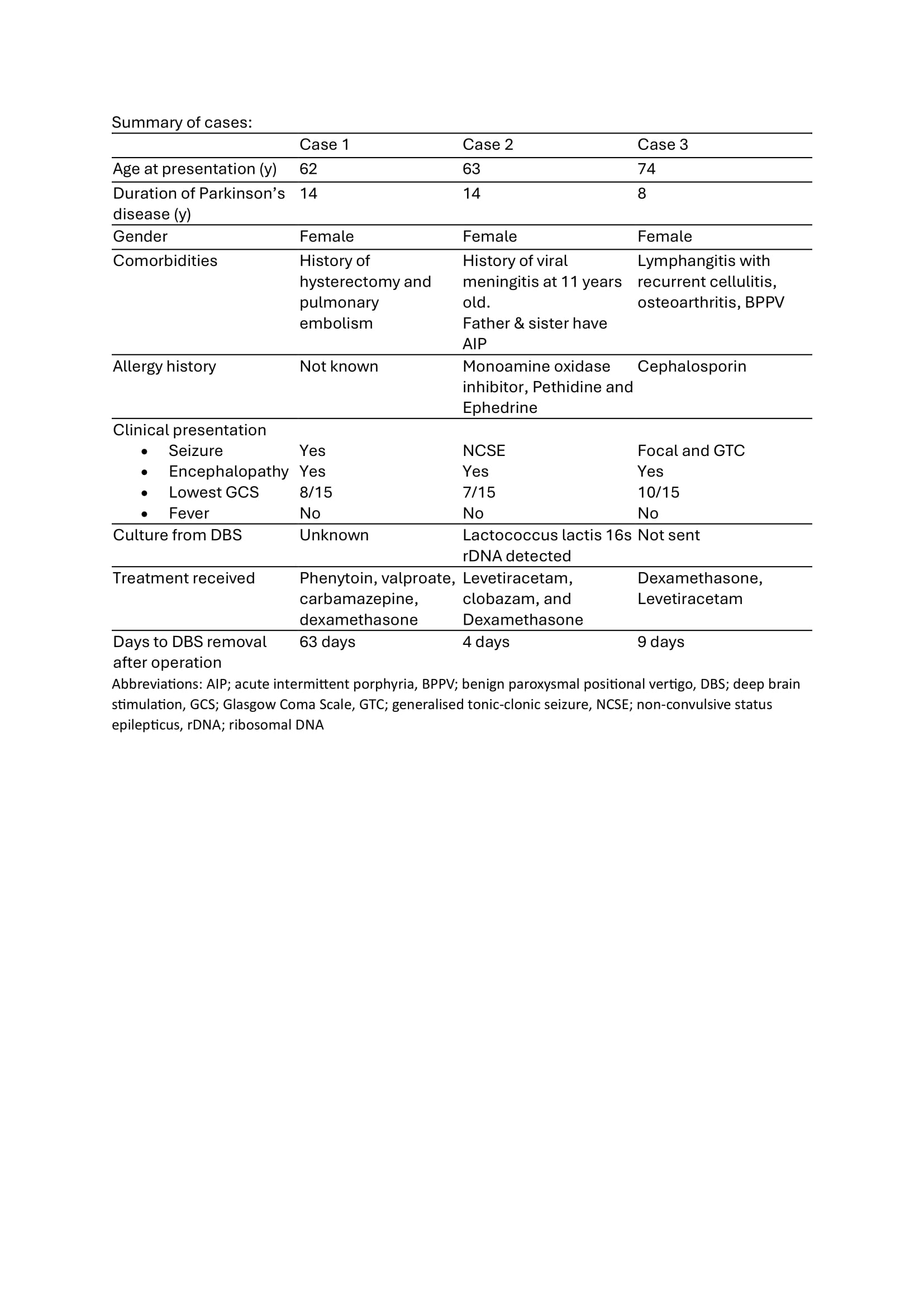
Table 1: Summary of Cases
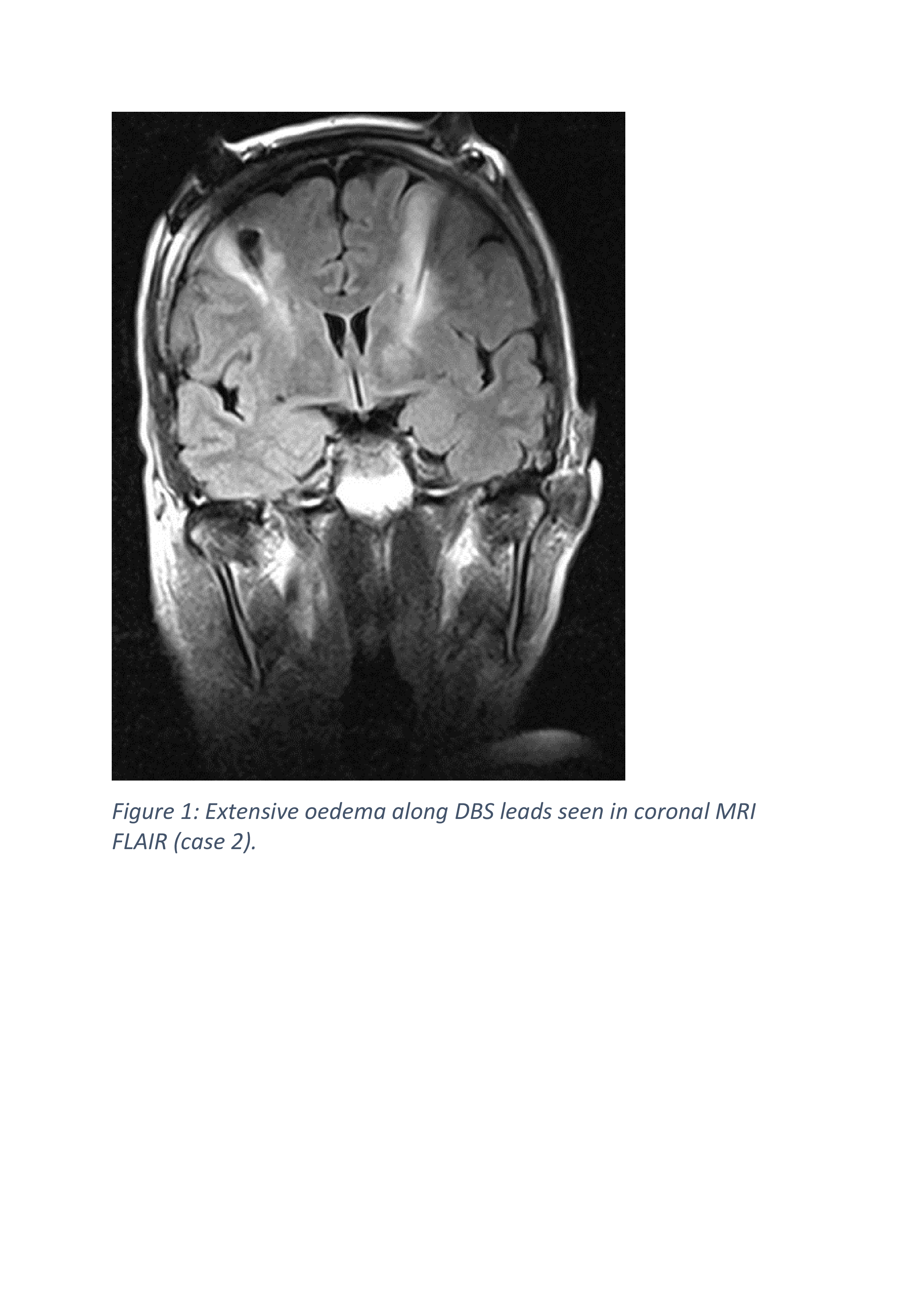
Figure 1

Figure 2
References: 1. Gulino, M., Kim, D., Pané, S., Santos, S. D., & Pêgo, A. P. (2019). Tissue response to neural implants: the use of model systems toward new design solutions of implantable microelectrodes. Frontiers in Neuroscience, 13. https://doi.org/10.3389/fnins.2019.00689
2. Kim JW, Hwang JH, Kim IK, Kim YE, Yang HJ, Ehm G, Kim HJ, Kim DG, Paek SH, Jeon BS. Acute brain reaction to DBS electrodes after deep brain stimulation: chronological observation. Acta Neurochir (Wien). 2013 Dec;155(12):2365-71; discussion 2371. doi: 10.1007/s00701-013-1853-3. Epub 2013 Sep 6. PMID: 24009047.
To cite this abstract in AMA style:
SS. Idris, O. Parras Granero, A. Chari, M. Krueger, H. Akram, J. Hyam, T. Foltynie, L. Zrinzo, P. Limousin. Symptomatic Peri-Lead Oedema After Bilateral Subthalamic Nucleus Deep Brain Stimulation Surgery- Not All Cases Are Self-Limiting: A Case Series [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/symptomatic-peri-lead-oedema-after-bilateral-subthalamic-nucleus-deep-brain-stimulation-surgery-not-all-cases-are-self-limiting-a-case-series/. Accessed July 6, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/symptomatic-peri-lead-oedema-after-bilateral-subthalamic-nucleus-deep-brain-stimulation-surgery-not-all-cases-are-self-limiting-a-case-series/