Category: Parkinson's Disease: Surgical Therapy
Objective: Evaluate GPi DBS as a rescue therapy for refractory dyskinesias and dystonia in long-term STN DBS patients.
Background: STN DBS effectively reduces medication dependency and improves motor function in PD. However, long-term use may lead to disabling dyskinesias and dystonia, often unresponsive to reprogramming or pharmacotherapy. GPi DBS has emerged as a potential rescue strategy for these patients. Technological advancements, such as multi-lead and independent current-controlled IPGs, allow for refined programming and expanded symptom coverage. Despite growing use, evidence on long-term efficacy remains limited.
Method: We retrospectively analyzed four PD patients with severe dyskinesias/dystonia after over ten years of bilateral STN DBS. All underwent GPi DBS implantation (unilateral or bilateral). Motor function was assessed using UPDRS III/IV, and quality of life with PDQ-39, at baseline and six months post-GPi DBS.
Results: GPi DBS led to a marked reduction in dyskinesias and improved quality of life. UPDRS IV decreased by 10-13 points, correlating with improved PDQ-39 scores. Patient 1’s UPDRS IV improved from 12 to 4, with PDQ-39 decreasing from 72 to 45. Patient 2’s UPDRS IV dropped from 14 to 5, with PDQ-39 from 75 to 48. Patient 3 showed UPDRS IV reduction from 20 to 7 and PDQ-39 from 80 to 50. Patient 4, with severe impairment, improved UPDRS IV from 17 to 6 and UPDRS III from 32 to 19, with PDQ-39 declining from 80 to 52. Improvement varied based on disease progression, residual dysfunction, and potential STN-GPi synergy.
Conclusion: GPi DBS effectively reduced dyskinesias and improved quality of life in STN DBS patients with refractory symptoms. The correlation between UPDRS IV and PDQ-39 underscores its clinical impact. Individualized treatment strategies are essential, considering disease heterogeneity, potential synergy with STN DBS, and technological advancements in DBS devices. Further studies with larger cohorts are needed to refine patient selection and optimize rescue DBS strategies.
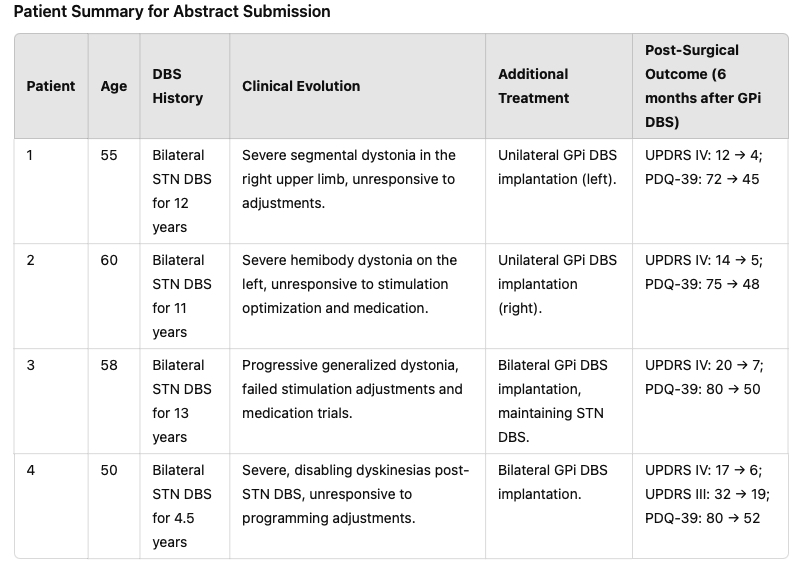
Patient Summary for Abstract Submission
References: Nagy AM, Tolleson CM. Rescue Procedures after Suboptimal Deep Brain Stimulation Outcomes in Common Movement Disorders. Brain Sci. 2016 doi: 10.3390/brainsci6040046.
Schnurman Z, Fazl A, Feigin AS, Mogilner AY, Pourfar M. Rescue Lead Implantation After Deep Brain Stimulation for Parkinson’s Disease: A Single-Center Experience and Case Series. Oper Neurosurg (Hagerstown). 2024 doi: 10.1227/ons.0000000000001142.
Cif L, Limousin P, Souei Z, Hariz M, Krauss JK. Alternative Deep Brain Stimulation Targets in the Treatment of Isolated Dystonic Syndromes: A Multicenter Experience-Based Survey. Mov Disord Clin Pract. 2025 . doi: 10.1002/mdc3.14324.
To cite this abstract in AMA style:
J. Brainer, P. Brainer, A. Brainer, S. Laurentino, R. Bandim, A. Oliveira, M. Cavalcanti, P. Brainer, C. Vidal. Rescue GPi DBS for Severe Dyskinesias and Dystonia in Long-Term STN DBS Parkinson’s Patients: A Case Series [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/rescue-gpi-dbs-for-severe-dyskinesias-and-dystonia-in-long-term-stn-dbs-parkinsons-patients-a-case-series/. Accessed July 6, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/rescue-gpi-dbs-for-severe-dyskinesias-and-dystonia-in-long-term-stn-dbs-parkinsons-patients-a-case-series/