Session Information
Date: Tuesday, September 24, 2019
Session Title: Drug-Induced Movement Disorders
Session Time: 1:45pm-3:15pm
Location: Agora 2 West, Level 2
Objective: To describe unusual cause of rhabdomyolysis in the two patients with Parkinson’s disease (PD).
Background: Levodopa-induced dyskinesia (LID) is usually seen in advanced stage of PD patients. Rhabdomyolysis associated with LID is rare but can be fatal.
Method: Case report and literature review
Results: Case 1: A 64-year-old man who was diagnosed PD for 7 years has had diphasic dyskinesia and motor fluctuation for two years. The patient took levodopa/benzeraside (LB) 750 mg/day, entacapone 500 mg/day, and piribedil 150 mg/day. Two days before admission, the patient increased the frequency of taking LB then developed severely generalized dyskinesia without fever. On admission, serum creatinine (Cr), potassium (K+), and aspartate aminotransferase slightly increased. Creatinine kinase (CPK) markedly elevated (4,246 U/L). Rhabdomyolysis associated with LID was diagnosed. The patient was hydrated. Diazepam 10 mg was given intravenously, and all antiparkinsonian medications were stopped. A few days later, dyskinesia gradually improved, and CPK returned to normal within five days. The patient was performed deep brain stimulation surgery which allowed him to reduce antiparkinsonian medications. The patient has never had severe dyskinesia since then. Case 2: A 61-year-old female who was diagnosed PD for 10 years has had motor complications for 6 years. Her currently took LB 800 mg/day, entacapone 800 mg/day, Madopar HBS 125 mg/day, and ropinirole 4 mg/day. Ropinirole was adjusted from 2 to 4 mg within the past month. Four days before admission, the patient experienced moderate dyskinesia which disturbed her activities of daily living. On admission, severely generalized dyskinesia which markedly presented on lower extremities without fever was observed. Cr and K+ slightly increased. CPK was markedly high (12,094 U/L). Rhabdomyolysis associated with LID was diagnosed. All anti-parkinsonian medications were stopped, and clonazepam 0.5 mg daily was given. A few days later, her symptoms were significantly improved and CPK decreased to normal within a week. On discharge, LB was decreased to 500 mg/day without resuming other medications.
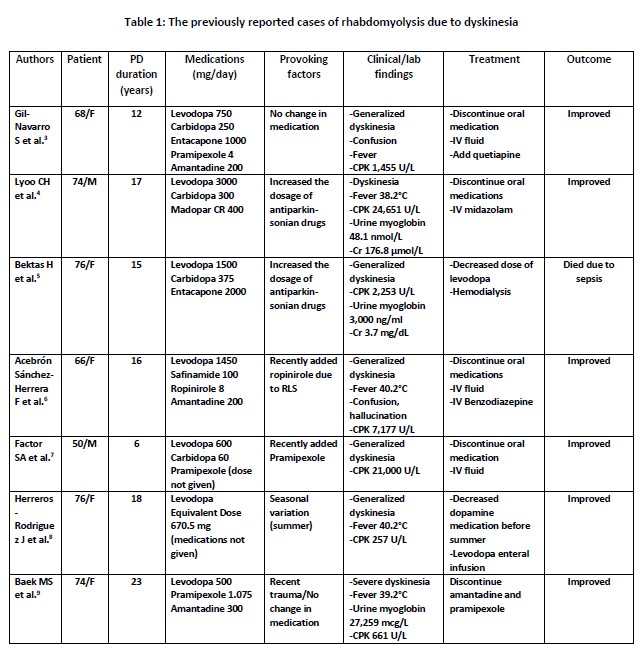
Conclusion: Rhabdomyolysis associated with LID is a rare life-threatening condition. Excessive dopaminergic administration was a major cause [table1]. Prompt recognition and treatment are recommended for favorable outcome.
References: 1. Zutt R, van der Kooi AJ, Linthorst GE, Wanders RJA, de Visser M. Rhabdomyolysis: review of the literature. Neuromuscul Disord. 2014;24:651-9. 2. Thanvi B, Lo N, Robinson T. Levodopa-induced dyskinesia in Parkinson’s disease: clinical features, pathogenesis, prevention and treatment. Postgrad Med J. 2007;83:384–8. 3. Gil-Navarro S, Grandas F. Dyskinesia–hyperpyrexia syndrome: another Parkinson’s disease emergency. Mov Disord.2010;25:2691-2. 4. Lyoo CH, Lee MS. Rhabdomyolysis induced by severe levodopa induced dyskinesia in a patient with Parkinson’s disease. J Neurol 2011;258:1893–4. 5. Bektas H, Deniz O, Temel S, Keklikoglu HD, Akyol S. Rhabdomyolysis related to dyskinesia in Parkinson’s disease. J Mov Disord. 2014;7:25-7. 6. Acebron Sanchez-Herrera F, Garcia-Barragan N, Estevez-Fraga C, Martinez-Castrillo JC, Lopez-Sendon Moreno JL. Dyskinesia-hyperpyrexia syndrome under continuous dopaminergic stimulation. Parkinsonism Relat Disord. 2017;36:103-4. 7. Factor SA, Molho ES. Emergency department presentations of patients with Parkinson’s disease. Am J Emerg Med. 2000;18:209-15. 8. Herreros-Rodriguez J, Sánchez-Ferro Á. Summertime dyskinesia-hyperpyrexia syndrome: the “dual heat” hypothesis. Clin Neuropharmacol 2016;39:210-211. 9. Baek MS, Lee HW, Lyoo CH. A patient with recurrent dyskinesia and hyperpyrexia syndrome. J Mov Disord. 2017; 10(3):154-157.
To cite this abstract in AMA style:
J. Srikajon, P. Srivanitchapoom, Y. Pitakpatapee, T. Sangpeamsook, C. Satukijchai, A. Suengtaworn. An unusual cause of rhabdomyolysis in the patients with Parkinson’s disease: A report of two cases [abstract]. Mov Disord. 2019; 34 (suppl 2). https://www.mdsabstracts.org/abstract/an-unusual-cause-of-rhabdomyolysis-in-the-patients-with-parkinsons-disease-a-report-of-two-cases/. Accessed April 2, 2026.« Back to 2019 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/an-unusual-cause-of-rhabdomyolysis-in-the-patients-with-parkinsons-disease-a-report-of-two-cases/