Objective: To describe the unusual clinical manifestations in a patient with coronavirus disease 2019 (COVID-19).
Background: Movement disorders are uncommon neurological manifestations of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Potential neurodegeneration might manifest later.
Method: Clinical observation and examination in a patient with COVID-19 related movement disorder.
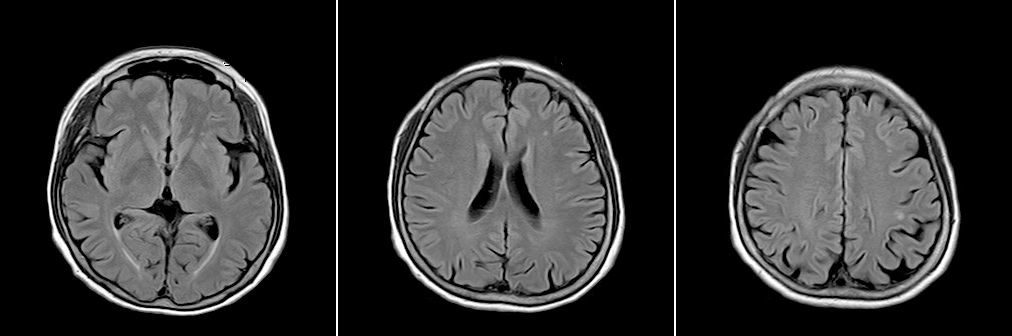
Results: This 63-year-old female has thrombocytosis, lumbar and cervical spine operation history and right-side breast cancer status post-operation and chemotherapy. She suffered from COVID-19 infection with the presentation of cough with sputum, rhinorrhea, and difficulty opening her eyes. She received molnupiravir for 5 days but progressive head, neck and upper trunk dystonia with tremor developed in the following months. Her symptoms did not respond obviously to oral clonazepam, trihexyphenidyl, baclofen, valproic acid even botulism injection. Brain magnetic resonance imaging showed nonspecific white matter lesions [figure1]. Cerebrospinal fluid (CSF) analysis showed mildly elevated protein without pleocytosis, malignant cell, or oligoclonal band, and IgG index was normal. Neuroimmunology tests were negative in CSF for NMDAR, AMPAR1, AMPAR2, CASPR2, LGI1, GABAbR antibodies and in serum for amphiphysin, CV2, PNMA2 (Ma2/Ta), Ri, Yo, Hu, Recoverin, SOX1, Titin, Zic4, and T4(DNER) antibodies. But serum anti-glutamic acid decarboxylase (GAD) 65 was positive. Malignancy and vasculitis workup were negative. Progressive mental decline, chest tightness, influent speech, and slow response developed. The mental test showed mild cognitive impairment. Electroencephalography was normal. Intravenous methylprednisolone 500mg was given for 5 days and then gradually tapered to the oral form. Her symptoms still persisted.
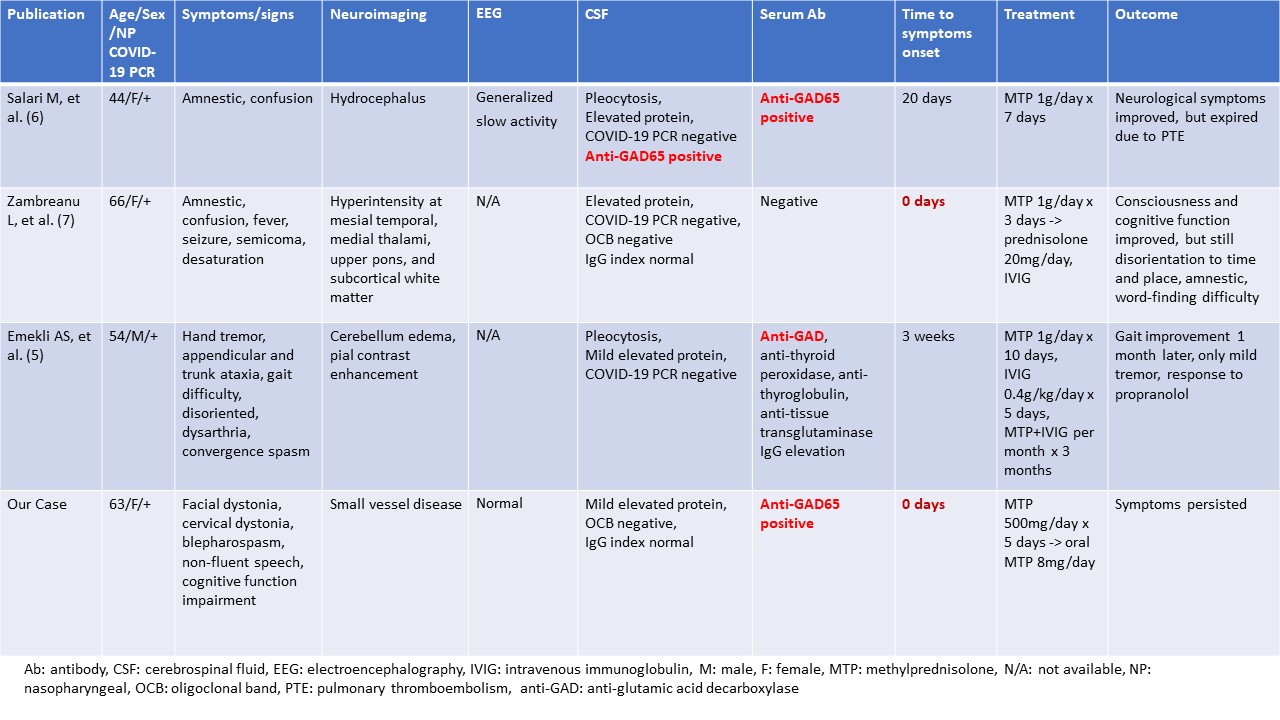
Conclusion: To our knowledge, it is rare to have movement disorders at the time of the onset of COVID-19 infection. Movement disorders of COVID-19 are rarely manifested as segmental dystonia. COVID-19 infection may trigger the production of autoantibody through immunological mimicry to target cell surface dopaminergic receptors in the basal ganglia or its connections, resulting in movement disorders or neurodegenerative diseases [table1]. Closely monitoring COVID-19 survivors for the possibility of post-COVID movement disorders is necessary.
References: [1] Paterson RW, et al. Brain 2020 Oct 1;143(10):3104-3120.
[2] Brandão PRP, et al. Tremor Other Hyperkinet Mov (N Y) 2021 Jul 8;11:26.
[3] Ghosh R, et al. Mov Disord Clin Pract 2021 Apr 28;8(5):669-680.
[4] Dade M, et al. Int J Mol Sci. 2020 May 24;21(10):3701.
[5] Emekli AS, et al. Neurol Sci. 2021 Oct;42(10):3995-4002.
[6] Salari M, et al. Clin Case Rep. 2022 Dec 12;10(12):e6597.
[7] Zambreanu L, et al. J Neurol Neurosurg Psychiatry. 2020 Nov;91(11):1229-1230.
To cite this abstract in AMA style:
PY. Chen. Anti-glutamic acid decarboxylase associated encephalitis presenting with new onset movement disorder after COVID-19 infection [abstract]. Mov Disord. 2023; 38 (suppl 1). https://www.mdsabstracts.org/abstract/anti-glutamic-acid-decarboxylase-associated-encephalitis-presenting-with-new-onset-movement-disorder-after-covid-19-infection/. Accessed July 10, 2026.« Back to 2023 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/anti-glutamic-acid-decarboxylase-associated-encephalitis-presenting-with-new-onset-movement-disorder-after-covid-19-infection/