Category: Parkinson's Disease: Surgical Therapy
Objective: To evaluate the short-term effects of deep brain stimulation (DBS) of the Globus Pallidus internus (GPi) versus the Subthalamic Nucleus (STN) on non-motor symptoms, psychiatric outcomes, and overall disease burden in Parkinson’s disease (PD) treated with neuromodulation.
Background: DBS is a well-established therapy for managing motor symptoms in PD, but the effects of different stereotactic targets on non-motor and psychiatric symptoms are less defined, particularly with pallidal stimulation, which may have distinct effects on non-motor domains. This study examined these differences using validated scales and longitudinal follow-up at 6 months
Method: We conducted a prospective, non-randomized, longitudinal study in PD patients managed at the University of Florida. Clinical and neuropsychiatric evaluations were performed at baseline, 3, and 6 months post-DBS implantation. Validated measures included the Non-Motor Symptoms Scale (NMSS), Unified Parkinson’s Disease Rating Scale (UPDRS I-IV, total score), Hamilton Depression Rating Scale (HDRS), Hamilton Anxiety Rating Scale (HAMA), SCOPA-AUT (autonomic dysfunction), and the Parkinson’s Disease Questionnaire (PDQ-39). Between-group comparisons were analyzed using Mann-Whitney U tests.
Results: Of 51 initially enrolled PD patients, 33 completed all required assessments (GPi: n=20; STN: n=13) (Table 1). All patients showed a reduction in baseline scores at 6 months. At this timepoint, STN-DBS patients exhibited a trend toward higher NMSS (median: 32.5 vs 8.0) and UPDRS total scores (median: 42.0 vs 24.0) compared with GPi-DBS, suggesting a greater symptom burden. STN-DBS was also associated with significantly higher depression (HDRS median: 2.5 vs 0.0, p=0.017) and anxiety scores (HAMA median: 3.0 vs 1.0, p=0.047) than GPi-DBS. No significant differences were observed in PDQ-39 scores (median: STN-DBS 17.5 vs GPi-DBS 8.0). Additionally, a trend toward improved autonomic dysfunction (SCOPA-AUT, median: STN-DBS 5.5 vs GPi-DBS 5.0) was noted in the STN-DBS group.
Conclusion: While both GPi and STN DBS improve motor function, STN-DBS was associated with higher neuropsychiatric scores in this cohort. Most non-motor scales showed overall improvement. Additional long-term controlled studies are needed, but treatment decisions should be individualized based on each patient’s motor and non-motor phenotypes.
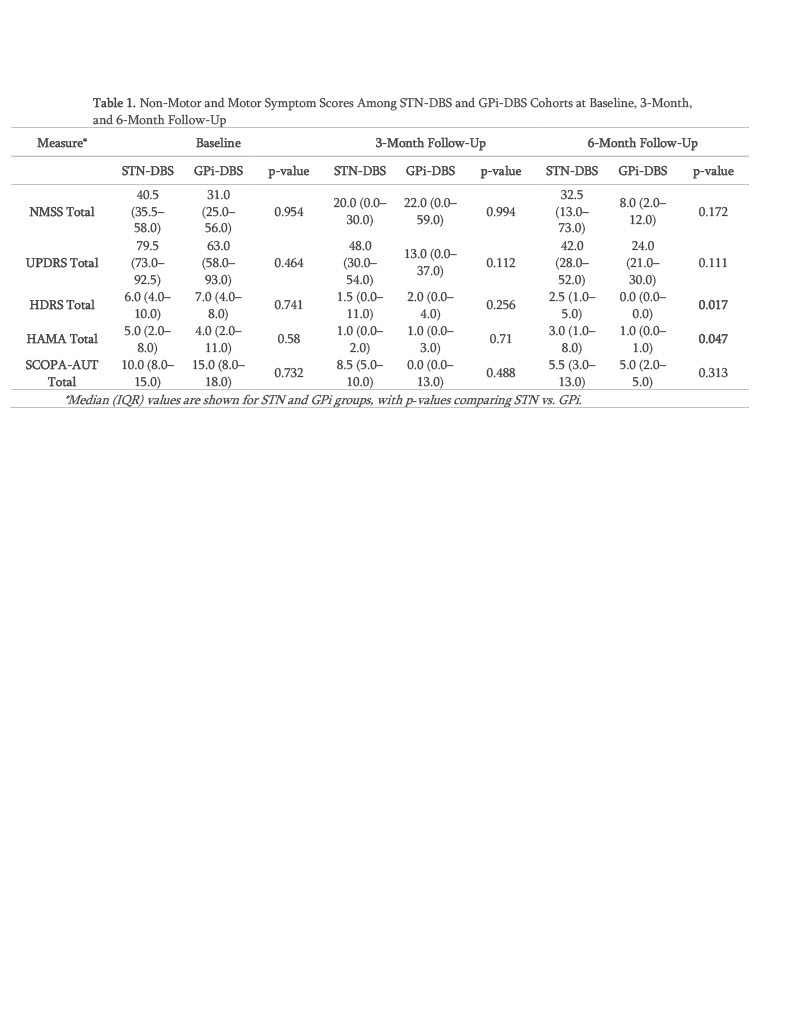
Table 1
To cite this abstract in AMA style:
G. Rodriguez Garcia, G. Hey, A. Martinez Nunez, J. Hilliard, A. Ramirez-Zamora. Are There Differences in Non-Motor Outcomes of Parkinson’s Disease Treated with GPi vs. STN Deep Brain Stimulation? [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/are-there-differences-in-non-motor-outcomes-of-parkinsons-disease-treated-with-gpi-vs-stn-deep-brain-stimulation/. Accessed April 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/are-there-differences-in-non-motor-outcomes-of-parkinsons-disease-treated-with-gpi-vs-stn-deep-brain-stimulation/