Category: Ataxia
Objective: to describe clinical features and diagnostic tests in a patient with Ataxia Telangiectasia (AT) in Vietnam.
Background: AT is a rare hereditary syndrome, the second most common autosomal recessive ataxia in children. The definitive diagnosis is established by either increased radiation-induced chromosomal breakage in cultured cells or progressive cerebellar ataxia with homozygous or compound heterozygous type mutations of the ATM gene.
Method: We report a clinical case diagnosed with AT but genetic testing results revealing a heterozygous mutation located on the ATM gene.
Results: A non-consanguineous 10-year-old male presented with cervical dystonia and gait difficulty lasting for a year. The onset began at the age of 6 with neck tremors and cursive handwriting, followed by left leg dragging after one year.
Upon examination, the patient presented cerebellar syndrome with dysarthria, gait ataxia, limb ataxia, and nystagmus. The patient also presented with generalized dystonia, most pronounced in the neck. Cognitive impairment was recorded. Muscle strength was normal, and no sensory disturbances. Pyramidal sign and autonomic nervous system disorders were sparing. The patient exhibited ocular telangiectasia [Figure 1] but no accompanying skin lesions. Brain MRI revealed mild cerebellar atrophy. Blood alpha-fetoprotein levels were elevated (662.6 ng/ml). Blood tests, liver and renal function, vitamin B12 and folate levels, vitamin E levels, and ceruloplasmin were within normal range. CSF analysis showed normal cytology and protein levels. Also, anti-MOG, and anti-aquaporin 4 were negative. Genetic testing using an ataxia panel revealed only one heterozygous mutation on the ATM gene at position chr11:108335911, confirmed by Sanger sequencing. However, our genetic testing did not rule out deletions and duplications, which the encounter rate is very low [1] and would require confirmation by MLPA technique, not available in Vietnam and excessively high cost.
Nevertheless, considering the early onset of cerebellar ataxia, associated retinal telangiectasia, cerebellar atrophy on MRI, and elevated AFP levels, this patient was diagnosed with possible AT according to the ESID Registry definition.
Conclusion: The diagnosis of AT by clinicians should rely on clinical symptoms and imaging studies, as accessibility genetic testing may not encompass all types of mutations.
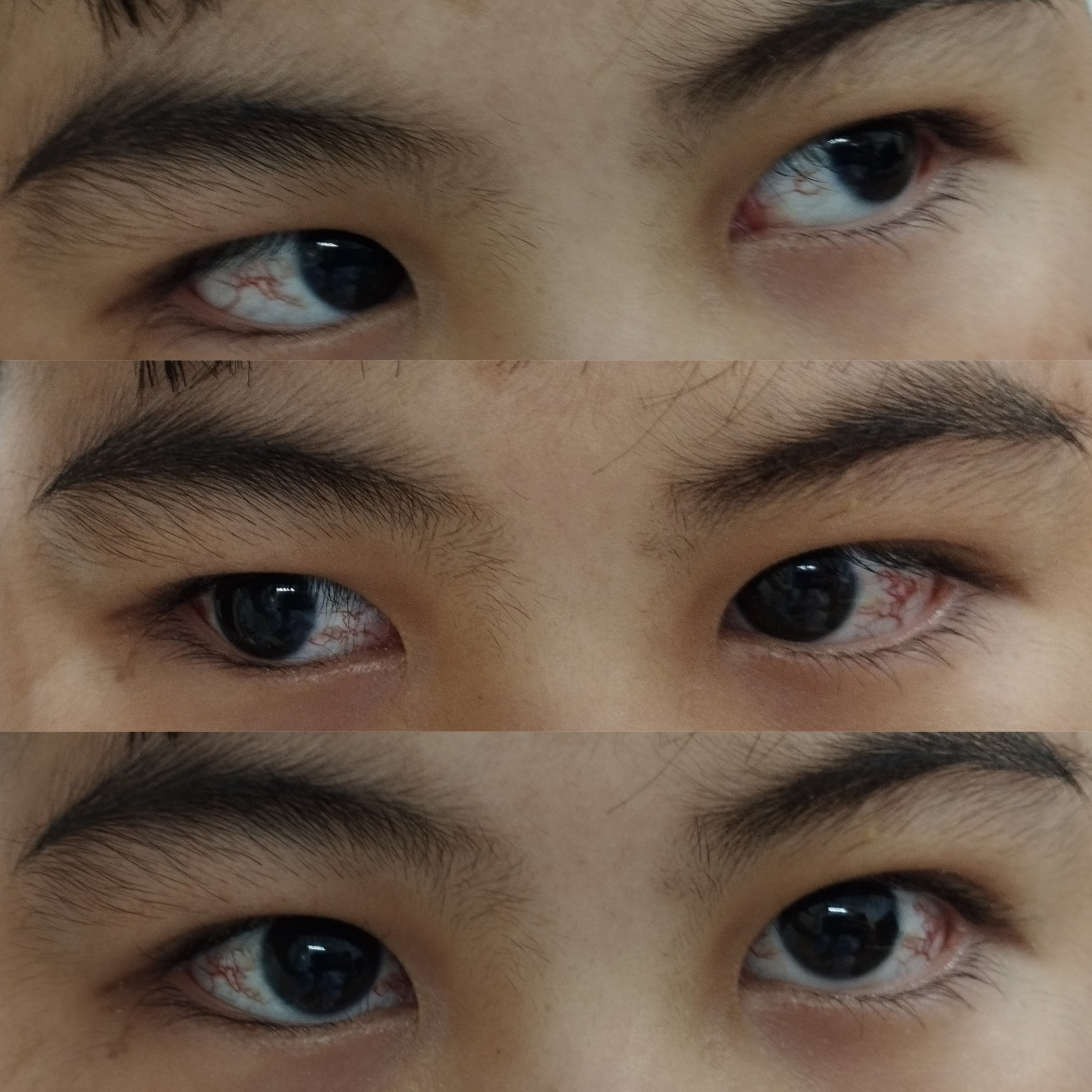
Figure 1. Ocular telangiectasia in both the eyes
References: [1] van Os NJH, Hensiek A, van Gaalen J, Taylor AMR, van Deuren M, Weemaes CMR, Willemsen MAAP, van de Warrenburg BPC. Trajectories of motor abnormalities in milder phenotypes of ataxia telangiectasia. Neurology. 2019 Jan 1;92(1):e19-e29. doi: 10.1212/WNL.0000000000006700. Epub 2018 Nov 30. PMID: 30504431.
To cite this abstract in AMA style:
H. Ngo Thi, T. Nguyen Anh. Ataxia Telangiectasia Diagnosis in Lower-Middle-Income Countries: A Case Report [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/ataxia-telangiectasia-diagnosis-in-lower-middle-income-countries-a-case-report/. Accessed July 7, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/ataxia-telangiectasia-diagnosis-in-lower-middle-income-countries-a-case-report/