Session Information
Date: Tuesday, September 24, 2019
Session Title: Parkinsonisms and Parkinson-Plus
Session Time: 1:45pm-3:15pm
Location: Agora 3 West, Level 3
Objective: We created a TMS protocol for paired-pulse cerebellar-M1 stimulation and repetitive cerebellar stimulation to augment cerebellar-brain inhibition and reduce postural instability in progressive supranuclear palsy (PSP).
Background: The cerebellum inhibits the motor cortex along the cerebello-thalamo-cortical pathway for normal postural reflexive motor control. This normal inhibition, called cerebellar-brain inhibition (CBI), is diminished in PSP (1, 2). Methods for targeting this pathway using paired-pulse cerebellar-M1 and cerebellar repetitive stimulation are inconsistent (3). Coil types used are variable, and MRI-guided stimulation (neuronavigation) is variably used.
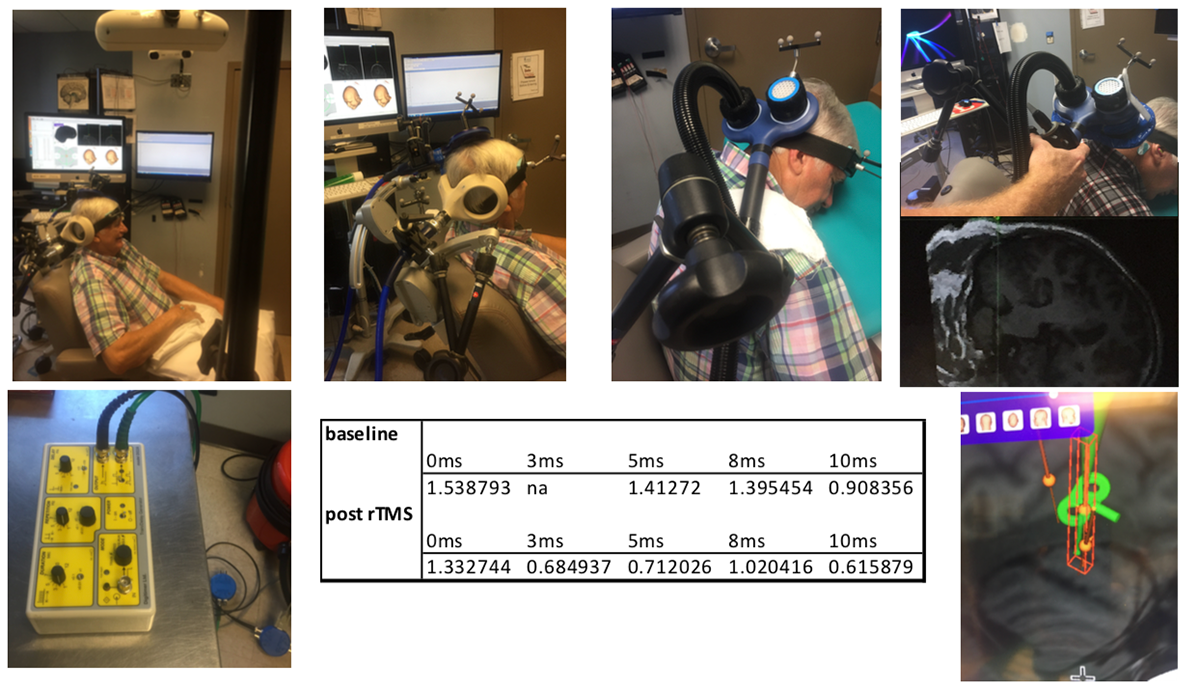
Method: We positioned a portable Polaris Vicra on an elevated tripod to the subject’s right. With Brainsight2 the camera was able to detect the subject tracker (positioned on a band in the right frontal region) and 2 coil trackers (figure-of-8 over the left M1 and double cone over the right cerebellum, each with bent bars rotated toward the camera). 2 arms were affixed to the back of the chair for the coils. Prior to CBI testing, resting motor thresholds (RMTs) with specific machine outputs were obtained from all 3 calibrated coils (70mm figure-of-8 with Magstim Bistim2 for the test pulse, 110mm double cone with Magstim Bistim2 for the cerebellar conditioning pulse, and 70mm air-cooled figure-of-8 coil with MagStim Rapid2 for rTMS treatment). For CBI the bistim was uncoupled and connected to a digimeter to deliver pulses at 90% RMT at 0, 3, 5, 8, and 10 ms. During extended cerebellar rTMS treatments the patient leaned forward on a firm wedge with his head turned to the right.
Results: After 10 4,000-pulse sessions of 10Hz cerebellar rTMS, the average motor evoked potential decreased from 1.41 to 0.71 at the 5ms cerebellar-M1 interstimulus interval, representing a 50% augmentation of CBI.
Conclusion: Augmenting cerebellar-brain inhibition in PSP is feasible and tolerable, but careful attention must be paid to tracker and camera orientation for consistent cerebellar and M1 targeting, and separate RMT measurement is needed for all coil types and stimulators used. Widely available cooled double cone coils and double cone sham coils are needed.
References: 1. Shirota Y, Hamada M, Hanajima R, Terao Y, Matsumoto H, Ohminami S, Tsuji S, Ugawa Y. Cerebellar dysfunction in progressive supranuclear palsy: a transcranial magnetic stimulation study. Mov Disord. 2010 Oct 30;25(2413-9). 2. Brusa L, Ponzo V, Mastropasqua C, Picazio S, Bonnì S, Di Lorenzo F, Iani C, Stefani A, Stanzione P, Caltagirone C, Bozzali M, Koch G. Theta burst stimulation modulates cerebellar-cortical connectivity in patients with progressive supranuclear palsy. Brain Stimul. 2014 Jan Feb;7(1):29-35. 3. Van Dun K, Bodranghien F, Manto M, Marien P. Targeting the cerebellum by noninvasive neurostimulation: a review. Cerebellum 2017 (16):695-741.
To cite this abstract in AMA style:
M. George, W. Devries, M. Dale. Cerebellar transcranial magnetic stimulation with neuronavigation for postural instability in PSP [abstract]. Mov Disord. 2019; 34 (suppl 2). https://www.mdsabstracts.org/abstract/cerebellar-transcranial-magnetic-stimulation-with-neuronavigation-for-postural-instability-in-psp/. Accessed July 8, 2026.« Back to 2019 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/cerebellar-transcranial-magnetic-stimulation-with-neuronavigation-for-postural-instability-in-psp/