Session Information
Date: Sunday, October 7, 2018
Session Title: Dystonia
Session Time: 1:45pm-3:15pm
Location: Hall 3FG
Objective: To describe a safe and well tolerated technique of botulinum toxin (BnTA) injection into the longus capitis muscle (LCM) in a patient with anterocaput in cervical dystonia.
Background: Cervical dystonia with anterocaput pattern is difficult to treat due to the profound position of the head flexors. The LCM, one of the main head flexors, is positioned prevertebral under the pharyngeal mucosa. Data about injection techniques of the LCM is scarce. A transcutaneous fluoroscopy guided approach to the adjacent longus colli muscle (1) and a pharyngeal endoscopy guided technique, injecting LCM based on morphological characteristics were described (2). Here, we describe a new technical approach combining rigid video-endoscopy and EMG, which was well tolerated and safe.
Methods: A 58 year old female patient with idiopathic cervical dystonia comprising torticollis and anterocaput pattern had persisting head flexion even after treatment with high doses of onaBnTA (600 units). The patient was settled in a half supine position. With a rigid endoscope (0°, Hopkins, Karl Storz, Germany) the pharyngeal wall was inspected and the LCM was identified. After topic anaesthesia an EMG-needle (75mm, 22G, natus MyoJect) was inserted under endoscopic sight and EMG signal was recorded during rest, phonation and slight flexion of the head (video provided with poster). Two treatment cycles with injection of 15 units and after 3 month 20 units onaBnTA were performed. The patient was evaluated before and 4 weeks after each injection. The dosage of the other percutaneously treated muscles remained unchanged.
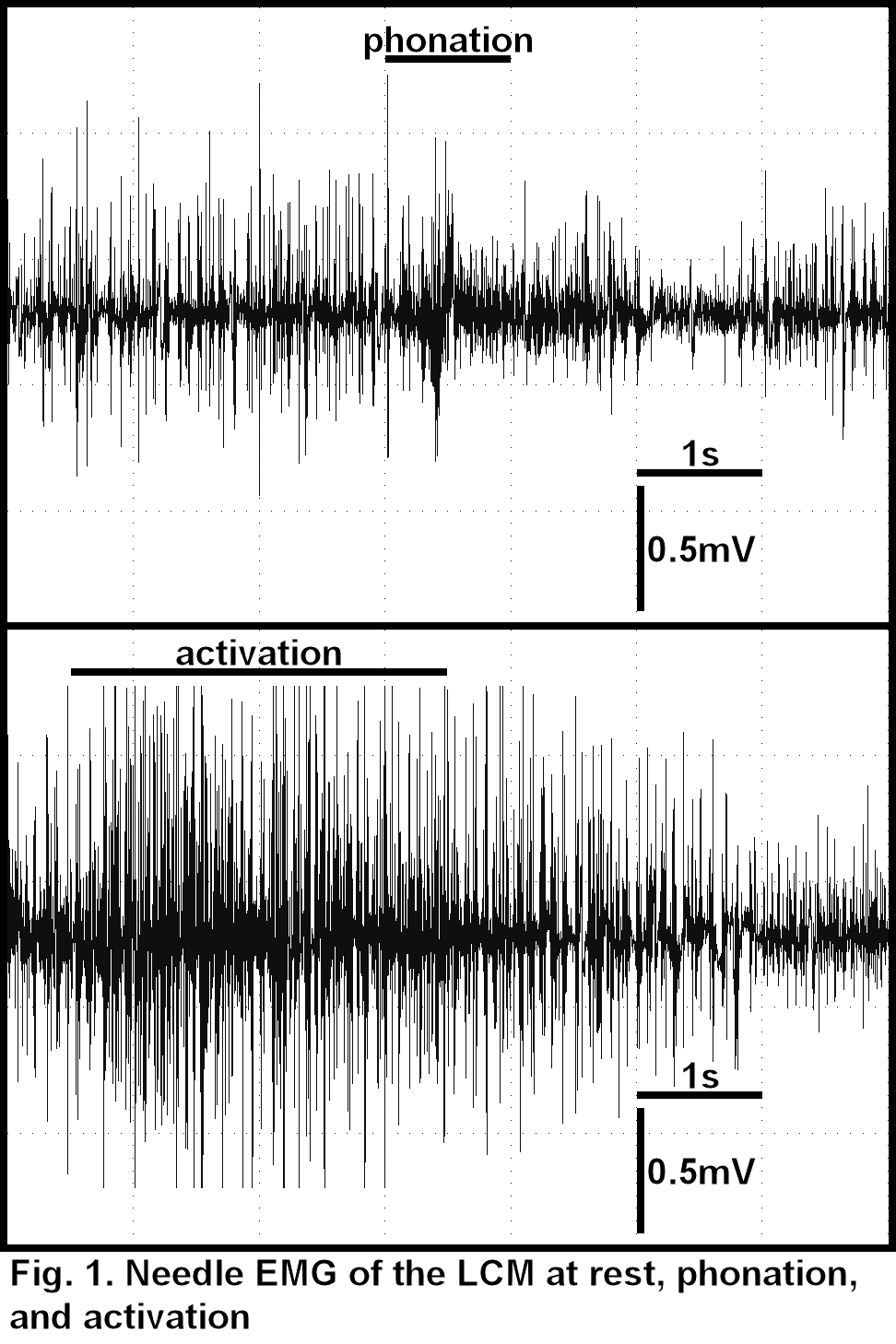
Results: EMG signal revealed a constant activation of the muscle at rest (dystonic activity), an increase during head flexion and no change of activity during phonation (Fig. 1). Both injections were well tolerated and not painful to the patient. On examination 4 weeks after treatment she reported less difficulties in lifting the head and a relevant reduction of head flexion. A significant but not yet complete improvement of antecaput was observed, documented by TWSTR-Scale (Torticollis Severity Sub-Scale: before 18 after 13/38 points).
Conclusions: Injection of LCM under guidance of rigid endoscopy and EMG is feasible, was well tolerated and led to improvement of anterocaput. EMG functionally identified the LCM. Compared to fluoroscopy, our technique is free of radiation. Compared to a transcutaneous EMG guided approach, the risk of damaging electrically inactive tissues such as arteries is low.
References: 1) Glass GA et al. Fluoroscopic, EMG-guided injection of botulinum toxin into the longus colli for the treatment of anterocollis. Park Rel Dis. 2009;15(8):610–3. 2) Reichel, G et al. Endoscopic-guided injection of botulinum toxin into the longus capitis muscle and into the obliquus superior part of the longus colli muscle in dystonic antecaput [abstract]. Mov Disord. 2016; 31 (suppl 2).
To cite this abstract in AMA style:
J. Michelis, F. Schuler, I. Debove, J. Müllner, L. Lachenmayer, E. Seifert. Combined EMG and endoscopy guided botulinum toxin injection of the longus capitis muscle in cervical dystonia with anterocaput [abstract]. Mov Disord. 2018; 33 (suppl 2). https://www.mdsabstracts.org/abstract/combined-emg-and-endoscopy-guided-botulinum-toxin-injection-of-the-longus-capitis-muscle-in-cervical-dystonia-with-anterocaput/. Accessed July 13, 2026.« Back to 2018 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/combined-emg-and-endoscopy-guided-botulinum-toxin-injection-of-the-longus-capitis-muscle-in-cervical-dystonia-with-anterocaput/