Session Information
Date: Tuesday, June 6, 2017
Session Title: Therapy in Movement Disorders
Session Time: 1:45pm-3:15pm
Location: Exhibit Hall C
Objective: To describe the occurrence, diagnostic approach, clinical management and outcome of diphasic dyskinesias (Dyskinesias-Improvement-Dyskinesias, DID) in a large group of Parkinson’s Disaese (PD) patients treated with levodopa carbidopa intestinal gel (LCIG).
Background: Levodopa carbidopa intestinal gel (LCIG), although widely adopted for treatment of Parkinson’s Disease (PD) motor fluctuations, still presents some limitations. In addition to the widely described device related adverse events, levodopa side effects are the main clinician concern. Evidences have suggested that LCIG is an effective treatment in overcome dyskinesias, however, no information are reported about the quality of targeted dyskinesias.
Methods: we adopted a retrospective chart review of LCIG patients seen at 4 movement disorder centers. Patients who experienced DID after LCIG titration were selected. The following data were recorded: motor diary, UPDRS IV and levodopa equivalent daily dose (LEDD) pre and post LCIG initiation, as well as strategy adopted to manage DID. The latter were categorized in order to propose a management algorithm.
Results: In our cohort 12% patients (16/131 subjects) reported DIDs after titration. All of them were treated with add-on therapies to levodopa before LCIG introduction. Biphasic dyskinesias were clinically detected at the early follow-up visit after titration, except in one case that manifested DID during the long term follow-up. The main red flag to suspect DIDs was the emergence of dyskinesias after lunch time or during the afternoon (end-of-dose). The most reported strategies adopted to overcome DID were: adopting a double flow infusion rate, decreasing/increasing the morning dose with a compensatory increase of the continuous infusion rate, infuse a higher extra dose bolus before lunch, re-establishing pre-existing oral therapies other than levodopa, and 24-hour infusion. Some of them required a caregiver intervention or multiple consultations that delayed titration time.
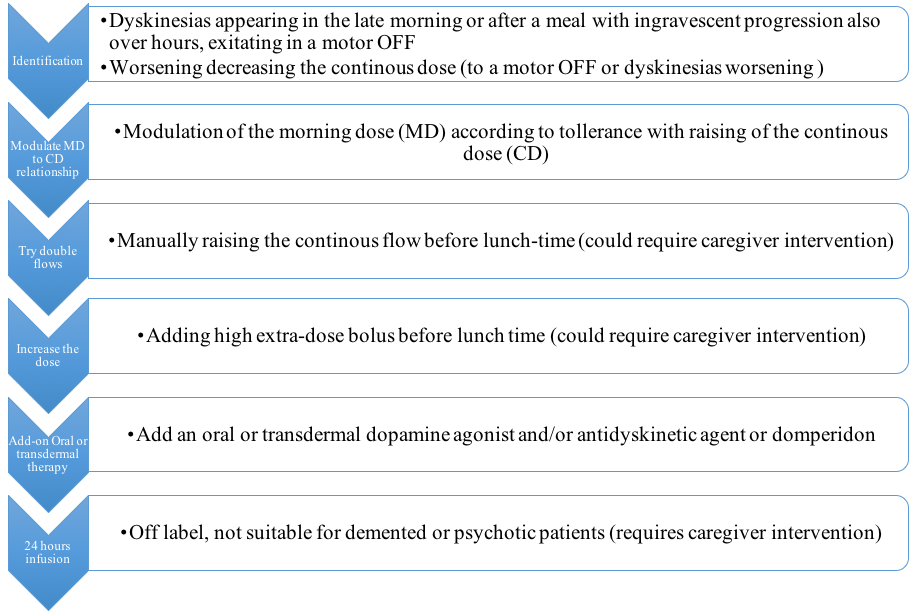
Conclusions: DID could significantly challenge LCIG titration and its overall outcome but their burden is still underestimated. In fact, they could also lead to treatment failure also when correctly recognized. Since a standardized tool (e.g. questionnaire) is still missing, we herein propose an algorithm that might guide clinicians towards DID recognition and treatment (Figure 1).
References: Fahn S. The spectrum of levodopa-induced dyskinesias. Ann Neurol. 2000;47:S2-9.
Antonini A, Fung VS, Boyd JT et al. Effect of levodopa-carbidopa intestinal gel on dyskinesia in advanced Parkinson’s disease patients. Mov Disord. 2016 Apr;31:530-537.
To cite this abstract in AMA style:
M. Marano, M. Marano, L. di Biase, R. Arca, G. Cossu, E. Coletta, V. Di Lazzaro, A. Fasano, P. Marano. Diphasic Dyskinesias during levodopa-carbidopa intestinal gel (LCIG) infusion: diagnosis and management in clinical practice. [abstract]. Mov Disord. 2017; 32 (suppl 2). https://www.mdsabstracts.org/abstract/diphasic-dyskinesias-during-levodopa-carbidopa-intestinal-gel-lcig-infusion-diagnosis-and-management-in-clinical-practice/. Accessed August 6, 2026.« Back to 2017 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/diphasic-dyskinesias-during-levodopa-carbidopa-intestinal-gel-lcig-infusion-diagnosis-and-management-in-clinical-practice/