Category: Huntington's Disease
Objective: Huntington’s Disease (HD) is an autosomal dominant neurodegenerative disorder resulting from an expansion of CAG trinucleotide repeats in the gene encoding the huntingtin protein.
Background: This expansion leads to a progressive decline characterized by a triad of symptoms: neuropsychiatric disturbances, choreoathetosis, and dementia. While symptom onset typically occurs in the fourth to sixth decade of life, variations in presentation and age of onset are recognized.
Method: Patient is a 31-year-old female who is adopted with a complex medical history including PTSD, ADHD, severe depression with previous suicidal thoughts, abusive relation and was left abandoned by husband and her son taken away by the father and her clear cell renal carcinoma (status post right nephrectomy at age 5), and motor vehicle accident 3 years ago with head concussion and loss of consciousness. Since the accident, she has exhibited progressive gait disturbance causing her to bump into objects, and have falls. She has severe choreoathetosis involving the face, neck, trunk, and extremities. Her memory deteriorated that she misplaced items, repetitively asked questions, and struggled with daily tasks like shopping. In terms of speech, she has dysarthria, word difficulty finding and semantic paraphasia. However, the patient lost the insight that she initially denied these deficits until she was showed the video evidence.
Results: Brain MRI showed a subjectively reduced volume of the caudate nuclei (arrow pointing to the right caudate nucleus) and putamina (arrowhead pointing to the right putamen) Axial T2-weighted image (Figure 1 A) and frontal horn width (FH)/intercaudate distance (CC) was 2.06 which is low. While the CC/inner table width (IT) ration was 0.13 which is elevated (Figure 1B). Genetic testing revealed 48 and 16 CAG repeats, with the 48-repeat allele in the fully penetrant range for Huntington’s Disease (HD). Patient received more social support and symptoms are managed by Valbenazine, clonidine, fluphenazine, duloxetine.
Conclusion: The delayed diagnosis of Huntington’s Disease in this young patient, due to confounding factors and initial psychiatric symptoms, underscores the importance of a comprehensive approach. This case serves to remind clinicians of the diverse clinical manifestations of HD and the need for early consideration in differential diagnoses.
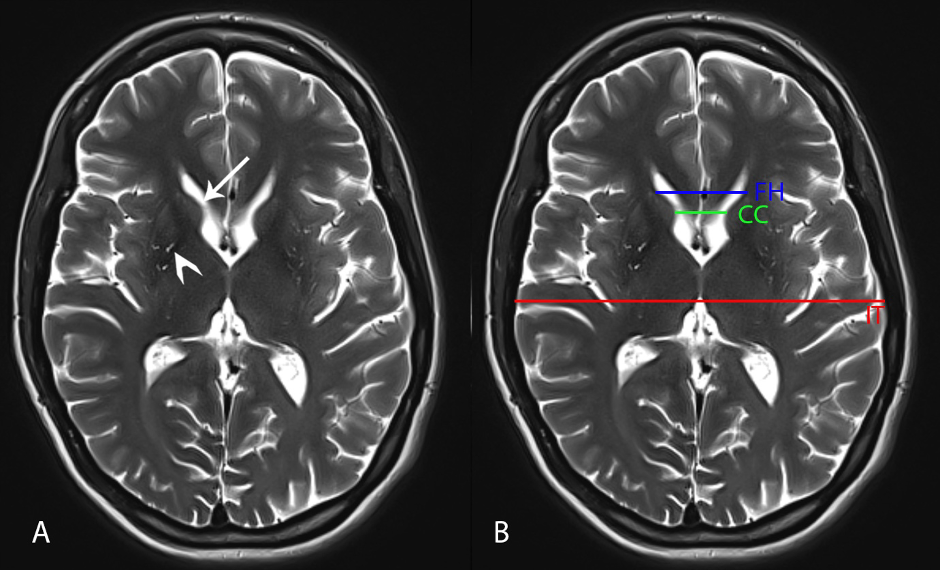
Figure 1: Brain MRI
To cite this abstract in AMA style:
A. Sim, A. Drozdov, D. Carrillo, L. Acosta. Huntington disease in a Patient with Extensive Psychiatric History [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/huntington-disease-in-a-patient-with-extensive-psychiatric-history/. Accessed April 7, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/huntington-disease-in-a-patient-with-extensive-psychiatric-history/