Category: Tremor
Objective: To describe a case of hyperkinetic movement disorder associated with papillary thyroid carcinoma, highlighting the diagnostic workup and therapeutic interventions.
Background: Paraneoplastic neurological syndromes are remote effects of malignancies not attributable to direct tumor invasion or metastasis. They often result from immune-mediated mechanisms triggered by the underlying neoplasm.[1] Movement disorders are being increasingly reported in the presentation of Autoimmune/Paraneoplastic Encephalitides. [2],[3]
Method: Case report
Results: A 38-year-old male developed tremors affecting the head and bilateral upper extremities two weeks after initiating escitalopram for anxiety. Head tremor had oscillations in vertical and horizontal planes. Upper extremities had Holmes tremor[4]–[6], 3–5 Hz in frequency, low-amplitude, seen at rest and action. Tremors persisted despite discontinuation of escitalopram. Magnetic Resonance Imaging showed extensive patchy, confluent T2 FLAIR signal abnormality involving bilateral basal ganglia, midbrain, and bilateral medial temporal lobes with punctate foci extending superiorly into the corona radiata, without gadolinium enhancement. This was stable on serial imaging. Cerebrospinal fluid (CSF) analysis showed oligoclonal bands and lymphocytic pleocytosis. Infectious, autoimmune, and paraneoplastic panels (serum and CSF) were negative except for minimally elevated Glutamic Acid Decarboxylase (GAD-65) antibodies in serum only. A PET scan identified increased uptake in left thyroid lobe, and histopathology from thyroidectomy confirmed papillary thyroid carcinoma. With imaging and serological workup suggesting paraneoplastic/autoimmune rhombencephalitis, immunotherapy with pulse steroids and plasma exchange was initiated without significant benefit. Intravenous immunoglobulin and cyclophosphamide provided limited neurological improvement. Tremors were refractory to multiple medication trials: head tremor responded to botulinum toxin injections, and trihexyphenidyl modestly improved upper extremity tremors. Over the next two years, he developed pseudobulbar affect and progressive gait instability, leading to walker-dependence.
Conclusion: Minimally elevated GAD65 autoantibodies isolated in serum were not believed to be contributing to his clinical presentation. [7] An association between papillary thyroid carcinoma and hyperkinetic movement disorders has not yet been documented in the literature.
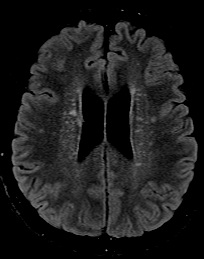
T2/FLAIR Hyperintensities Bilateral Corona radiata
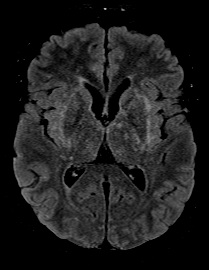
Bithalamic and Basal Ganglia FLAIR Hyperintensity
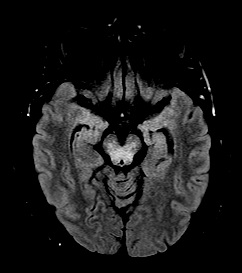
Midbrain and Bitemporal T2/FLAIR Hyperintensities
References: [1] F. Graus et al., “Updated Diagnostic Criteria for Paraneoplastic Neurologic Syndromes.,” Neurol. Neuroimmunol. neuroinflammation, vol. 8, no. 4, Jul. 2021, doi: 10.1212/NXI.0000000000001014.
[2] B. Balint, “Autoimmune Movement Disorders.,” Continuum (Minneap. Minn)., vol. 30, no. 4, pp. 1088–1109, Aug. 2024, doi: 10.1212/CON.0000000000001455.
[3] B. Balint, A. Vincent, H.-M. Meinck, S. R. Irani, and K. P. Bhatia, “Movement disorders with neuronal antibodies: syndromic approach, genetic parallels and pathophysiology.,” Brain, vol. 141, no. 1, pp. 13–36, Jan. 2018, doi: 10.1093/brain/awx189.
[4] G. HOLMES, “ON CERTAIN TREMORS IN ORGANIC CEREBRAL LESIONS,” Brain, vol. 27, no. 3, pp. 327–375, Jan. 1904, doi: 10.1093/brain/27.3.327.
[5] G. B. Raina et al., “Holmes tremor: Clinical description, lesion localization, and treatment in a series of 29 cases.,” Neurology, vol. 86, no. 10, pp. 931–938, Mar. 2016, doi: 10.1212/WNL.0000000000002440.
[6] K. P. Bhatia et al., “Consensus Statement on the classification of tremors. from the task force on tremor of the International Parkinson and Movement Disorder Society.,” Mov. Disord., vol. 33, no. 1, pp. 75–87, Jan. 2018, doi: 10.1002/mds.27121.
[7] B. Balint, K. P. Bhatia, and J. Dalmau, “‘Antibody of Unknown Significance’ (AUS): The Issue of Interpreting Antibody Test Results.,” Mov. Disord., vol. 36, no. 7, pp. 1543–1547, Jul. 2021, doi: 10.1002/mds.28597.
To cite this abstract in AMA style:
U. Agarwal, R. Al-Hader, S. Fu, Z. Farzal, M. Cerghet. Hyperkinetic Movement Disorder associated with Papillary Thyroid Carcinoma [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/hyperkinetic-movement-disorder-associated-with-papillary-thyroid-carcinoma/. Accessed April 7, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/hyperkinetic-movement-disorder-associated-with-papillary-thyroid-carcinoma/