Session Information
Date: Wednesday, June 7, 2017
Session Title: Ataxia
Session Time: 1:15pm-2:45pm
Location: Exhibit Hall C
Objective:
Objective: To report clinical, imaging and genetic findings in a case of ARSACS from India
Background: ARSACS was described initially from Quebec, Canada, and later from few other countries, but there is no clinical report of a genetically proven case from India. We report a case from Western India with typical clinical and imaging features, that was subsequently found to harbor a novel duplication in the SACS gene.
Methods: Clinical, imaging and genetic descriptive Case report
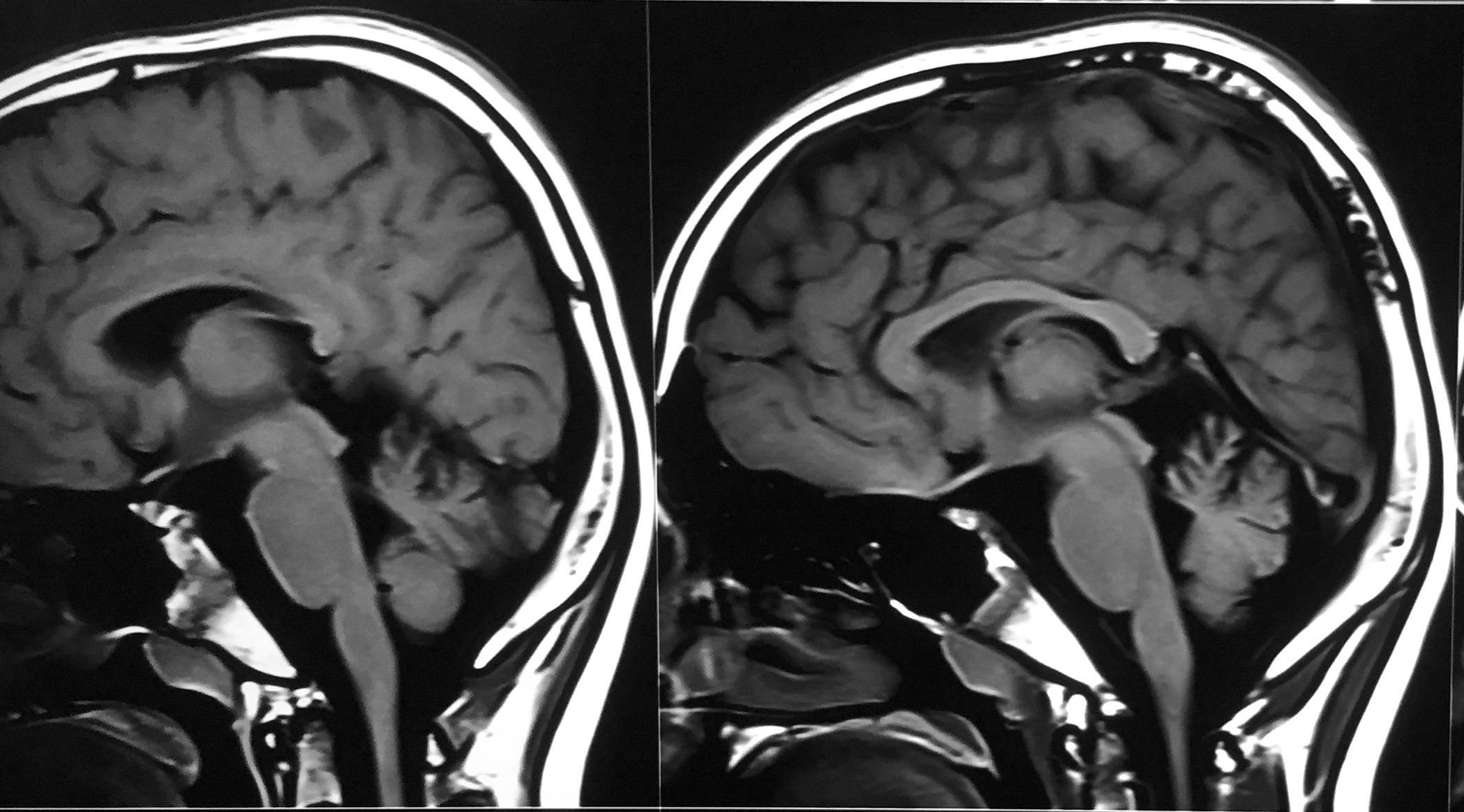
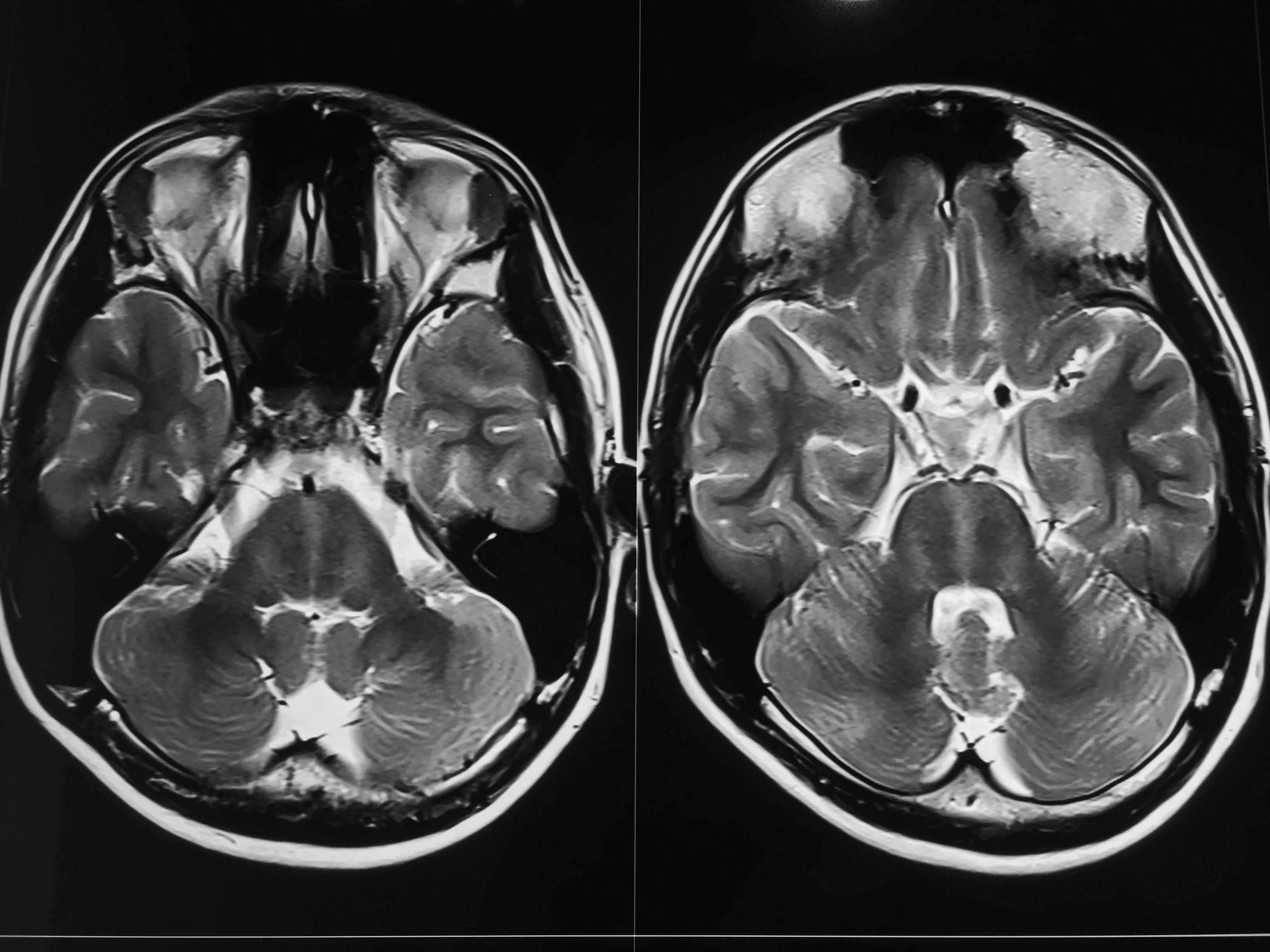
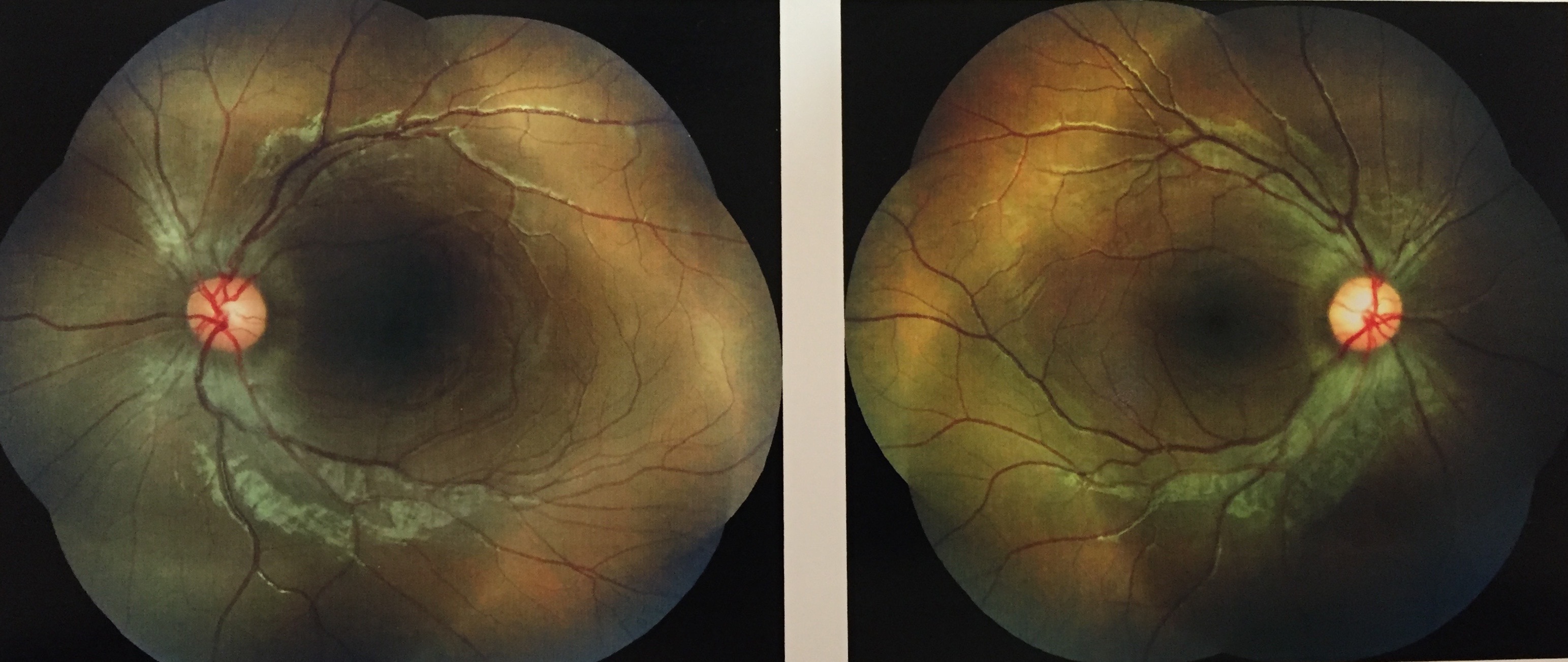
Results: A 12-year old boy presented with difficulty walking and poor balance since age 4, mild delay in reaching motor milestones and poor scholastic performance. Family history was negative , with no parental consanguinity. Extraocular movements were abnormal with saccadic pursuit, and normal saccades. Speech had a spastic and ataxic quality. Dysmetria and ataxia were present in upper limbs. Gait was ataxic, with difficulty walking tandem. Pes cavus was present. Deep tendon reflexes were absent in legs. Biochemical workup for alternative causes of ataxia was negative, as was gene testing for FA. MRI showed cerebellar superior vermian atrophy [Figure 1], linear ‘striped’ pontine hypointensities [Figure 2], and thickened middle cerebellar peduncles. EMG showed severe axonal and demyelinating neuropathy in all limbs, with absent SNAPs in legs, reduced CMAPs and low velocities. Funduscopic examination revealed myelinated nerve fibers radiating from optic disc and embedding retinal vessels. [Figure 3] Optical coherence tomogram showed thickening of retinal nerve fiber layer.
Targeted gene testing for a SACS gene mutation showed a homozygous four base pair duplication in exon 10 of the gene (chr13:23906322-23906325dupTCAC; Depth: 419x) that resulted in a frameshift and premature truncation of the protein 2 amino acids downstream to codon 3898 (p.Asp3898GlufsTer2; ENST00000382298) that was of pathogenic significance. The parents were both heterozygous for the same four-base pair duplication, providing further proof of pathogenicity.
Conclusions: This first clinical and genetically confirmed report of Indian ARSACS reinforces the view that this rare inherited ataxia has a typical, possibly unique combination of clinical, electrophysiologic, and imaging findings that can alert clinicians to the diagnosis in young-onset recessive ataxia.
References:
- Duquette A, Brais B, Bouchard JP, Mathieu J. Mov Disord. Clinical presentation and early evolution of spastic ataxia of Charlevoix-Saguenay. 2013 Dec;28(14):2011-4.
- Martin MH, Bouchard JP, Sylvain M, St-Onge O, Truchon S. Autosomal recessive spastic ataxia of Charlevoix-Saguenay: a report of MR imaging in 5 patients. AJNR Am J Neuroradiol. 2007 Sep;28(8):1606-8.
To cite this abstract in AMA style:
P. Agarwal. Indian ARSACS (Autosomal Recessive Spastic Ataxia of Charlevoix- Saugenay): Clinical report of the first genetically proven case from India, due to a novel SACS duplication [abstract]. Mov Disord. 2017; 32 (suppl 2). https://www.mdsabstracts.org/abstract/indian-arsacs-autosomal-recessive-spastic-ataxia-of-charlevoix-saugenay-clinical-report-of-the-first-genetically-proven-case-from-india-due-to-a-novel-sacs-duplication/. Accessed June 23, 2026.« Back to 2017 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/indian-arsacs-autosomal-recessive-spastic-ataxia-of-charlevoix-saugenay-clinical-report-of-the-first-genetically-proven-case-from-india-due-to-a-novel-sacs-duplication/