Objective: To evaluate medication safety strategies implemented to reduce medication errors in an i-MINC Program
Background: Medication mismanagement may lead to critical patient harm in people with Parkinson’s Disease (PD).1 About 70% of neurologists report hospitalized PD patients do not properly receive medications.2 Furthermore, only 50% of admissions had time-critical medications ordered correctly on hospitalization.3 The Parkinson’s Foundation published hospital care standards to avoid preventable harm to those with PD.1 As part of the i-MINC model, various strategies have been adopted to ensure safe and accurate medication administration. We aim to assess the effectiveness of these strategies.
Method: A retrospective chart review was performed on all patients admitted from home to the i-MINC Program at Glen Cove Hospital from January 1, 2024 – December 31, 2024. Those admitted from facilities or not diagnosed with PD were excluded. The following strategies were implemented and later assessed for compliance: (1) Medication reconciliation performed by a clinical pharmacist with the patient or caretaker prior to admission. (2) Non-formulary medications identified for procurement or provided by patient. (3) PD medications ordered by a clinical pharmacist in a custom fashion according to patients’ at-home regimen prior to patient arrival. (4) Medications deemed as contraindicated per the Parkinson’s Foundation evaluated [Table 1]. (5) PD medications supplied via automated dispensing cabinet. (6) Bar Code Medication Administration (BCMA) used. (7) Annual PD-specific medication training to all nurses on the i-MINC unit. (8) Transitions of care include medication prior authorization and bedside medication delivery.
Results: A total of 114 patients were admitted with 40% (n=46) admitted from home. Medication reconciliation was performed by a clinical pharmacist prior to admission in 98% (45/46) of patients. All PD medications were ordered in a custom fashion (46/46). None of the contraindicated or potentially harmful medications evaluated were ordered. BCMA compliance was 95.8% (158145/165066) for all medications on the i-MINC unit [Figure 1].
Conclusion: The strategies adopted by the i-MINC program at Glen Cove Hospital in coordination with clinical pharmacy have been compliant with standards to avoid preventable harm. Future directions include assessment of medication administration times.
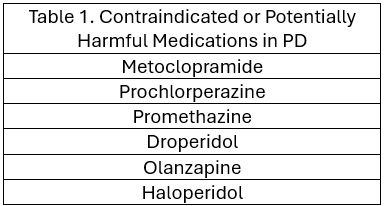
Table 1
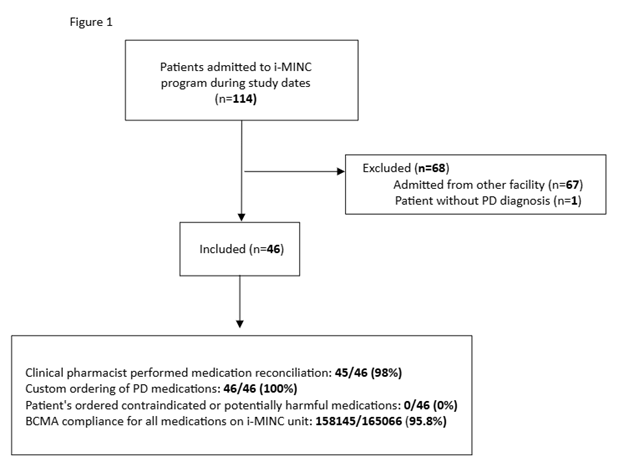
Figure 1
References: 1. Pronovost P, Azmi H, Okun MS, Walter B, Brooks A, Rosenfeld S. Protecting Parkinson’s Patients: Hospital Care Standards to Avoid Preventable Harm. Jt Comm J Qual Patient Saf. 2024 Dec;50(12):890-892. doi: 10.1016/j.jcjq.2024.08.004. Epub 2024 Nov 18. PMID: 39562228.
2. Viudez-Martínez A, Ramírez-López A, López-Nieto J, Climent-Grana E, Riera G. Antiparkinsonian Medication Reconciliation as a Strategy to Improve Safety by Preventing Medication Errors. Mov Disord Clin Pract. 2023 May 23;10(7):1090-1098. doi: 10.1002/mdc3.13789. PMID: 37476316; PMCID: PMC10354616.
3. Generali J. Optimizing Inpatient Care for Patients With Parkinson Disease. Hosp Pharm. 2024 Nov 29:00185787241299964. doi: 10.1177/00185787241299964. Epub ahead of print. PMID: 39619885; PMCID: PMC11607712.
To cite this abstract in AMA style:
N. Yousefzadeh, L. Hom, A. Defrank, M. Mccrossin, L. Rubin. Medication Error Reduction Strategies in an In-patient Multimodal Intensive Neurorehabilitation and Care (i-MINC) Program [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/medication-error-reduction-strategies-in-an-in-patient-multimodal-intensive-neurorehabilitation-and-care-i-minc-program/. Accessed April 5, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/medication-error-reduction-strategies-in-an-in-patient-multimodal-intensive-neurorehabilitation-and-care-i-minc-program/