Objective: To ascertain and delineate the differences in Levodopa Equivalent Dose (LEDD) among Parkinson’s disease (PD) subtypes and to examine its evolution over the disease’s trajectory.
Background: Parkinson’s Disease (PD) is a neurodegenerative disorder characterized by motor symptoms such as tremor, rigidity, and bradykinesia. These motor symptoms are managed mainly through dopaminergic medications. With the progression of PD, there is a concomitant increase in the required dosage of these medications to maintain motor function. However, this escalation in dopaminergic medication often correlates with the onset of adverse side effects. The Levodopa Equivalent Dose (LEDD) is a composite measure that quantifies the total intake of dopaminergic medications, considering both their strengths and dosages. Therefore, LEDD serves as a crucial indicator and metric for the progression of PD.
Method: We used data from Parkinson’s Progression Markers Initiative (PPMI, www.ppmi-info.org) to conduct this retrospective study. We evaluated PD patients who had available data on medication (Levodopa Equivalent Dose, LEDD) and Movement Disorder Society Unified Parkinson’s Disease Rating Scale part III motor score (UPDRS-III). Individuals who had undergone Deep Brain Stimulation (DBS) were excluded from analysis. Classification of PD patients into motor subtypes—Tremor Dominant, Akinetic Rigid, and Mixed—was conducted in accordance with the criteria outlined in [1]. We calculated the mean LEDD for each PD subtype indexed by the years since PD diagnosis (YSPDD). A two-way Analysis of Variance (ANOVA) was performed to assess the variance of LEDD across the PD subtypes over time and the corresponding interactions.
Results: 570 patients were included for analysis in this study ( 176 tremor dominant, 362 akinetic rigid, 32 mixed). The mean (SE) of LEDD at each YSPDD per PD subtype is plotted in [figure 1]. Our two-way ANOVA detected that both PD motor subtype and time since PD diagnosis independently impact LEDD (p < 0.0001 for both main effects) and that these effects were not dependent on each other (p > 0.05).
Conclusion: As PD progresses there is an expected increase in LEDD over time. The observed variability in the change of LEDD over time is contingent upon the motor subtype, underscoring the necessity for tailoring medication adjustments to individual patient profiles.
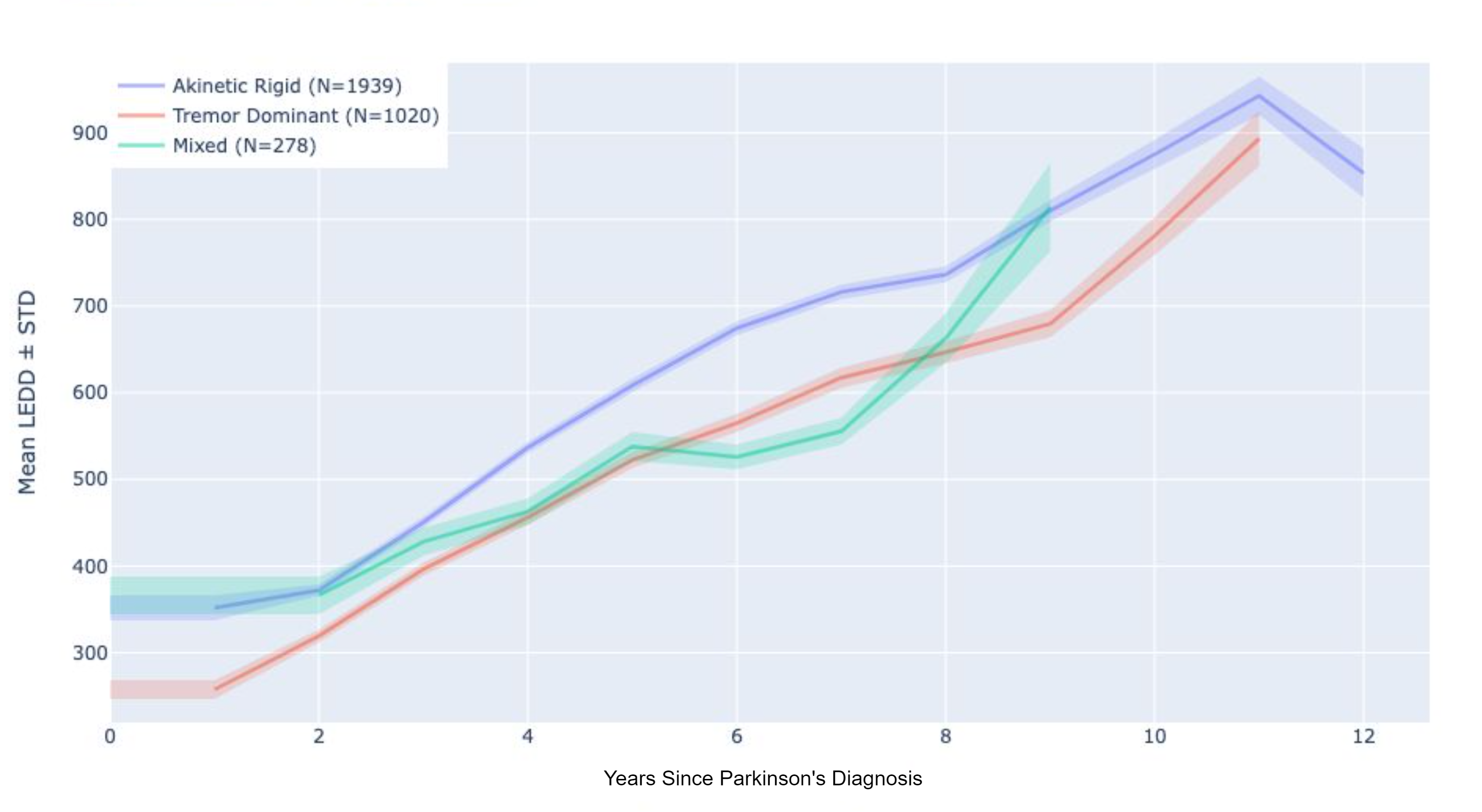
Change in LEDD among PD motor subtypes across time
References: [1] Adams, C., Suescun, J., Haque, A., Block, K., Chandra, S., Ellmore, T. M., & Schiess, M. C. (2023). Updated Parkinson’s disease motor subtypes classification and correlation to cerebrospinal homovanillic acid and 5-hydroxyindoleacetic acid levels. Clinical Parkinsonism & Related Disorders, 8, 100187.
To cite this abstract in AMA style:
V. Lavu, J. Dwarampudi, Q. Yuan, F. Sarmento, T. de Araujo, V. Garg, J. Wong. One dose fits all? An analysis of the levodopa equivalent dose over time in Parkinson’s disease [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/one-dose-fits-all-an-analysis-of-the-levodopa-equivalent-dose-over-time-in-parkinsons-disease/. Accessed August 3, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/one-dose-fits-all-an-analysis-of-the-levodopa-equivalent-dose-over-time-in-parkinsons-disease/