Objective: To gain an understanding from physicians on the impact of non-medical toxin switching (NMTS) in the treatment of movement disorders and other chronic conditions for which at least one botulinum toxin (BoNT) is indicated.
Background: NMTS occurs when decision makers within hospital systems, payors, or clinics force a BoNT switch to an alternative based off a false perception of interchangeability between BoNTs with a misperceived cost savings1. Data has demonstrated the negative impact of non-medical switching on patients with chronic conditions; however, the impact of NMTS specifically has yet to be examined2.
Method: This is a cross-sectional, exploratory web-based survey of US-based physicians who have experienced NMTS for which at least one BoNT is indicated. Physicians were recruited through email based off list servers from patient advocacy organizations, health systems, and institutions. Outcomes from physician survey data included impact on their treatment management approach and relationship with patients.
Results: Fifty physicians completed the survey and reported using BoNT for the treatment of cervical dystonia (92%), spasticity (86%), and blepharospasm (88%). Physicians reported feeling frustrated (82%) and uncertain (42%) due to NMTS. Additionally, 62% had to adjust the BoNT dosage due to NMTS, and 71% of these physicians administered subsequent dose adjustments. For physicians who did not change dosage due to NMTS, 10.5% reported a change in injection paradigm (i.e., number and/or location of sites). Nearly all surveyed physicians (96%) spent additional time counseling patients regarding the medication switch, and 50% spent additional time educating themselves on the new toxin. Over half of physicians (64%) submitted appeals to block NMTS, with 62.5% of them being successful. Moreover, 50% of physicians reported their patients had negative treatment experiences or outcomes due to NMTS. Additionally, 34% of physicians noted a negative impact on the physician/patient relationship; of these, 41% noted that NMTS was beyond their control and “not a physician-driven decision” [Table 1].
Conclusion: This survey suggests NMTS results in additional time burden to the physician, modification to dose and therapeutic application which required subsequent dose adjustments overtime, and a negative impact on the physician-patient relationship. NMTS may disrupt patient care and disease state management.
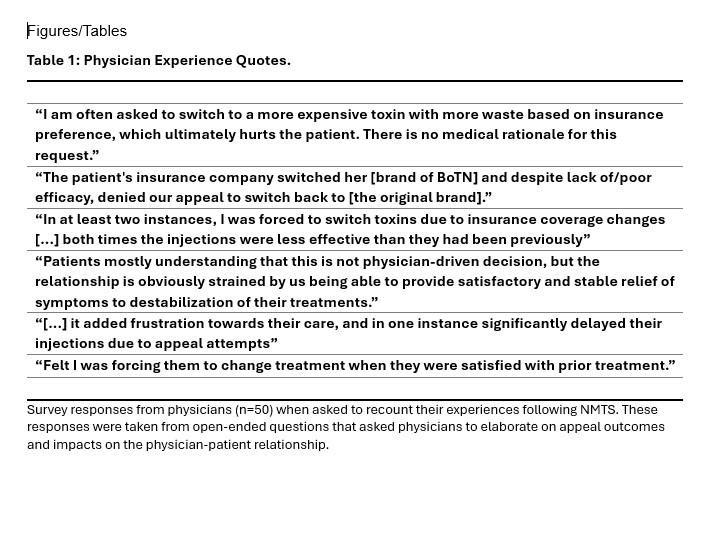
Table 1: Physician Experience Quotes
References: 1. Alliance for Patient Access. Non-Medical Switching and Botulinum Toxins. Available at:
https://www.patientaccesscollaborative.org/policy-papers/2018/12/13/botulinum-neurotoxins-and-non-medical-switching. Accessed June 19, 2021.
2. Alliance for Patient Access. A Study of the Qualitative Impact of Non-Medical Switching. Available at: https://www.patientaccesscollaborative.org/policy-papers/2019/3/7/a-study-of-the-qualitative-impact-of-non-medical-switching. Accessed on June 19, 2021.
To cite this abstract in AMA style:
P. Charles, L. Venditti, M. Nelson, R. Singh, K. Pazira, H. Kling, L. Kopaeva, S. Sharp, K. Harper. Physician Assessment of Non-Medical Toxin Switching on Patient Care [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/physician-assessment-of-non-medical-toxin-switching-on-patient-care/. Accessed April 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/physician-assessment-of-non-medical-toxin-switching-on-patient-care/