Objective: To define motor progression subphenotypes in Parkinson’s disease (PD) and evaluates the predictive power of clinical and smartphone data in distinguishing slow from fast progressors at baseline.
Background: PD exhibits heterogeneous motor progression, complicating treatment strategies. While clinical assessments like the Movement Disorder Society–Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) are standard, digital tools such as smartphone sensors offer novel insights into real-time motor changes. Few studies integrate these modalities to define subphenotypes or predict trajectories, a gap this analysis addresses using trial data.
Method: We conducted an exploratory analysis of 103 PD participants from the Exenatide-PD trial, tracked over 96 weeks in ON- and OFF-medication states. Adjusted mean changes in MDS-UPDRS Part III scores from baseline to week 96 were compared between exenatide and placebo across prespecified subgroups (sex, age, disease duration, motor subphenotypes like tremor-dominant or akinetic-rigid) and data-driven clusters (slow vs fast progressors). Predictive models integrated baseline MDS-UPDRS Part III scores with smartphone-derived metrics (e.g., gait, tremor). Accuracy was evaluated using area under the receiver operating characteristic curve (AUC) with 95% confidence intervals (CIs).
Results: In ON states, exenatide vs placebo differences in MDS-UPDRS Part III changes ranged from -0.03 (95% CI, -2.97 to 2.91) in females to 9.87 (95% CI, 8.10 to 11.64) in fast progressors. In OFF states, differences spanned 1.71 (95% CI, -0.92 to 4.34) in akinetic-rigid participants to 8.23 (95% CI, 5.91 to 10.55) in fast progressors. Data-driven fast progressors exhibited significantly greater decline (P<.001). Baseline prediction with MDS-UPDRS Part III alone yielded AUCs of 0.54 (95% CI, 0.00 to 0.93) ON and 0.53 (95% CI, 0.21 to 0.85) OFF; integrating smartphone data improved AUCs to 0.77 (95% CI, 0.39 to 1.00) ON and 0.76 (95% CI, 0.47 to 0.98) OFF. A simulated digital protocol combining both classifiers achieved AUCs of 0.74 (95% CI, 0.61 to 0.86) ON and 0.80 (95% CI, 0.67 to 0.91) OFF.
Conclusion: Motor progression in PD varies across subphenotypes, with data-driven fast progressors showing marked decline. Combining clinical and smartphone data enhances baseline prediction of motor trajectories, offering potential for personalized PD management.
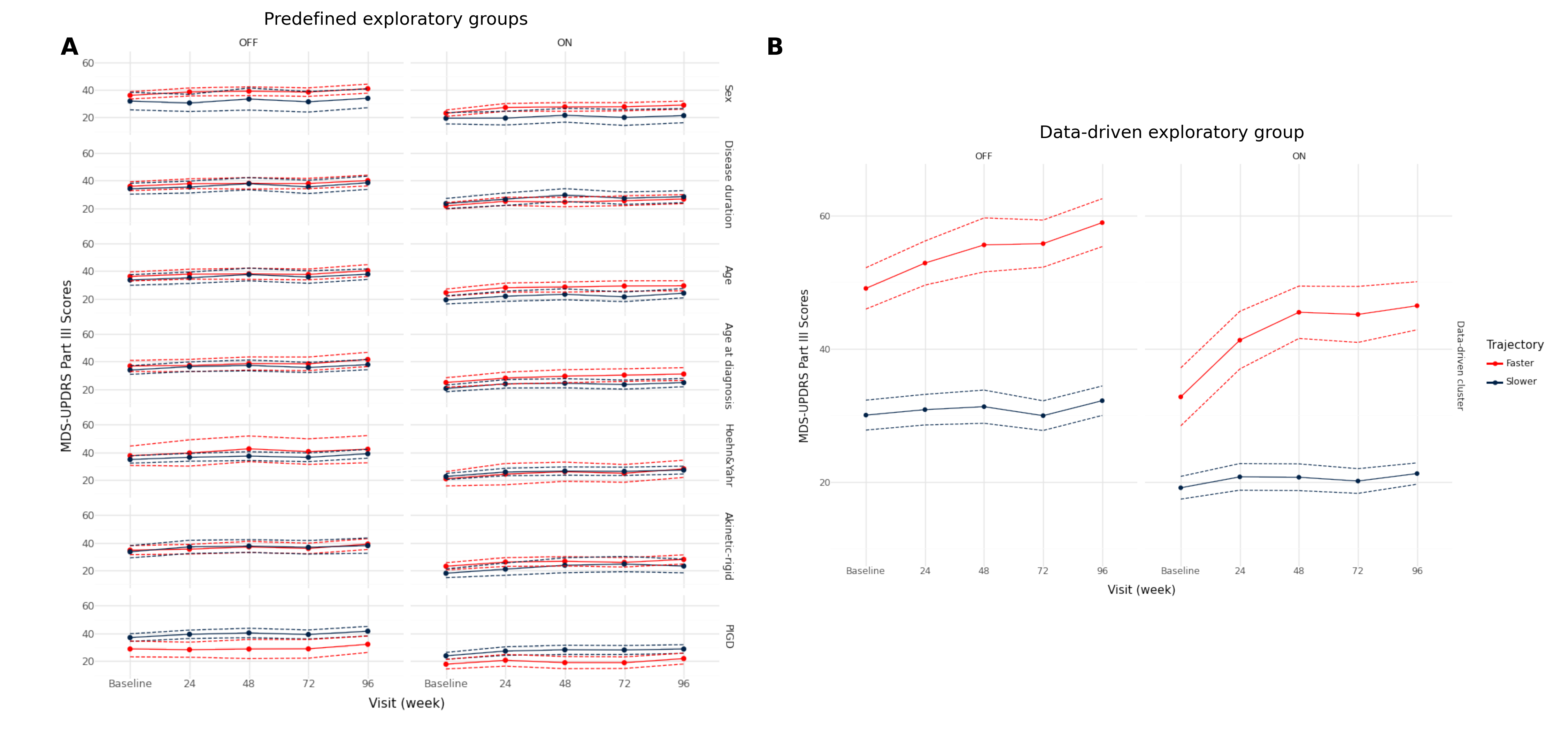
Figure 1
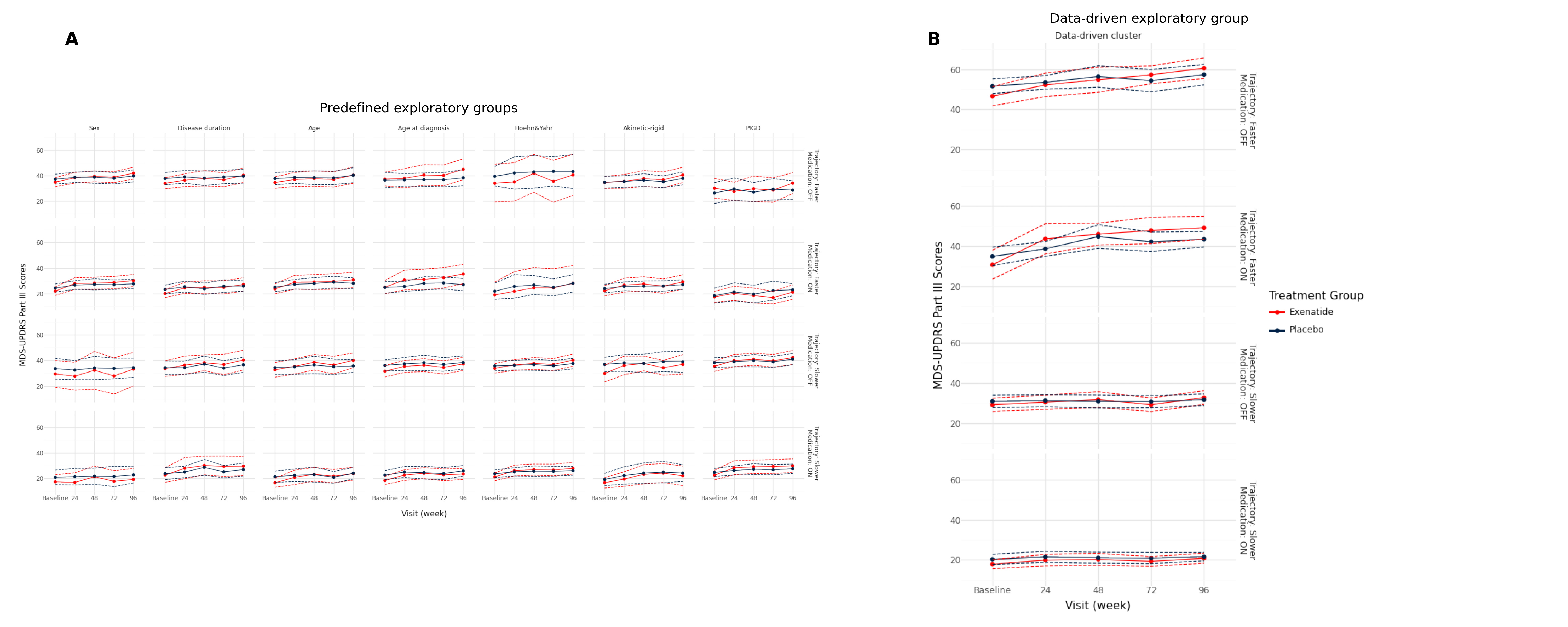
Figure 2
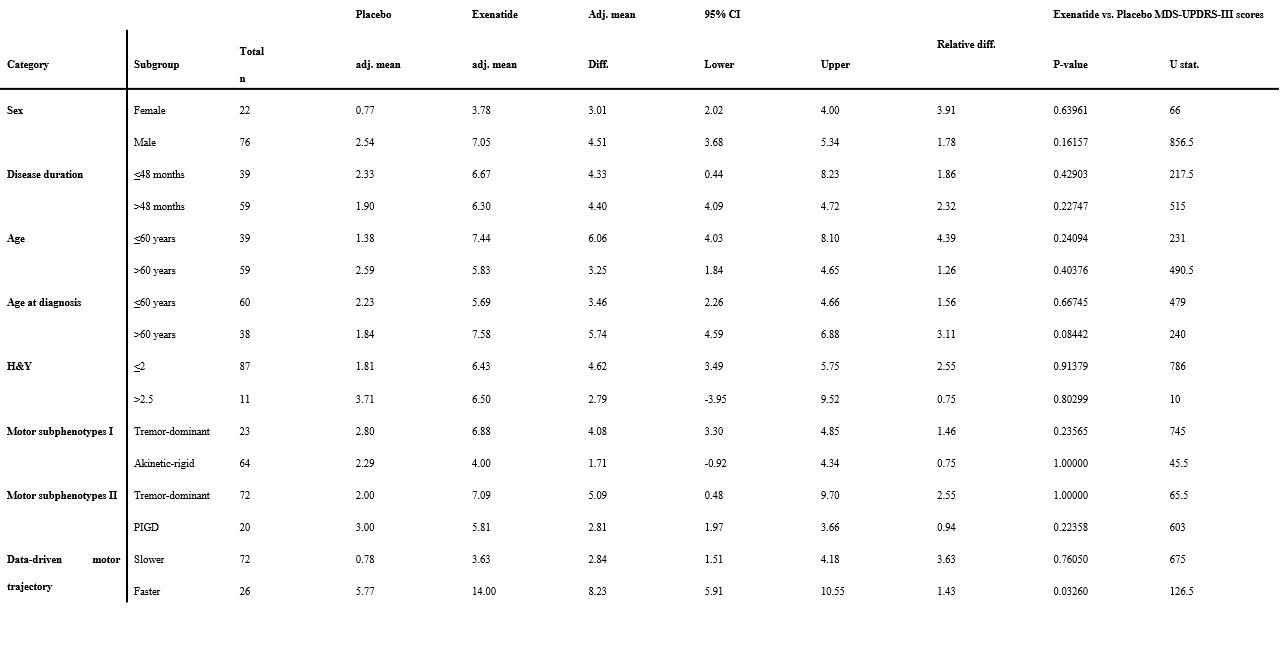
Table 2
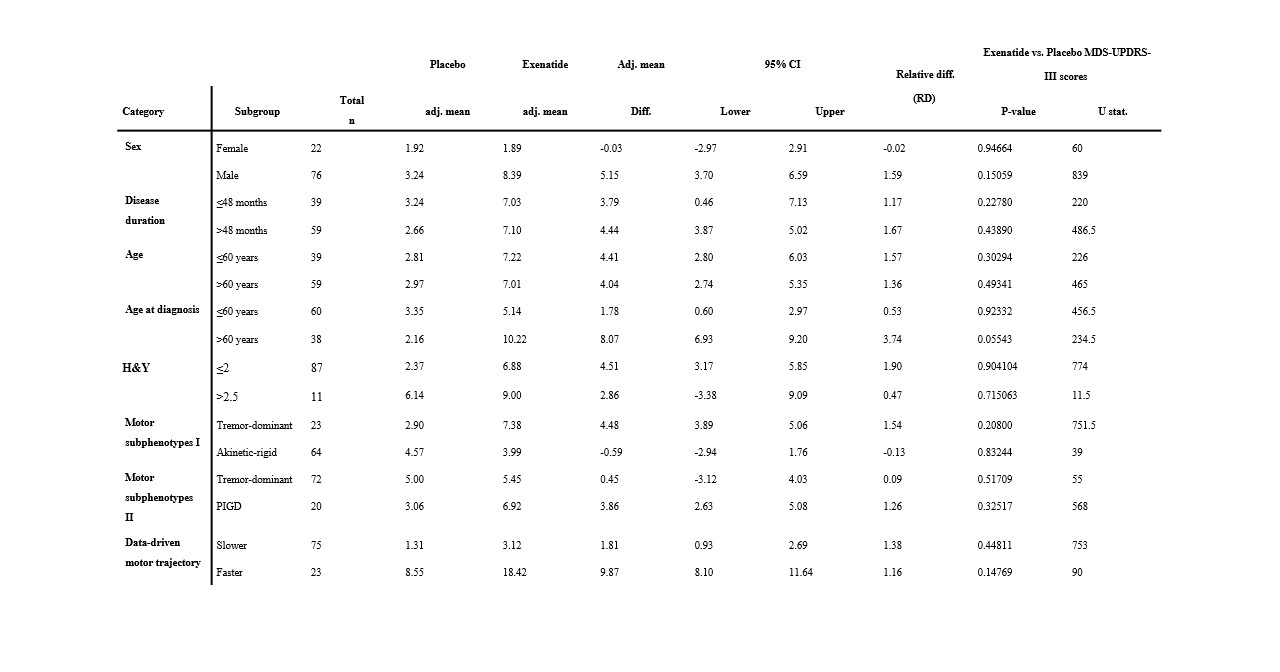
Table 3
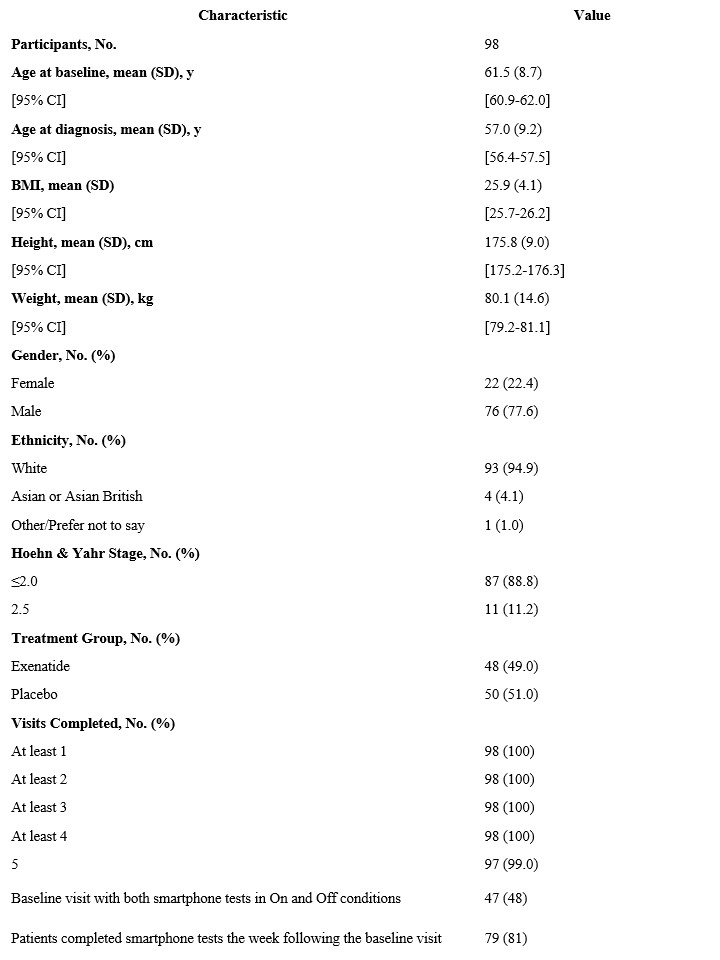
Table 1
To cite this abstract in AMA style:
T. Aubourg, K. Gunter, C. Lo, J. Welch, K. Groenewald, J. Klein, J. Razzaque, L. van Hillegondsberg, PL. Ratti, A. Nastasa, G. Auld, R. Mccomish, A. King, K. Chowdhury, N. Vijiaratnam, C. Girges, T. Foltynie, S. Arora, M. Hu. Predicting Parkinson’s Disease Motor Progression Using Clinical and Digital Data [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/predicting-parkinsons-disease-motor-progression-using-clinical-and-digital-data/. Accessed April 7, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/predicting-parkinsons-disease-motor-progression-using-clinical-and-digital-data/