Session Information
Date: Sunday, October 7, 2018
Session Title: Dystonia
Session Time: 1:45pm-3:15pm
Location: Hall 3FG
Objective: Introduction Rapid onset dystonias are uncommon.Common causes are drugs, post-stroke dystonia, or metabolic causes like hypo/hyperglycemia,hypocalcemia or hypomagnesemia
Background: Case presentation 11 year boy with normal antenatal history, mild delay in motor milestones had normal scholastic performance.He had a seizure and on regaining consciousness, started having left upper limb (Lt-UL) dystonia.After 10-15 days, he started having uncontrollable flinging movements of the left lower limb.He was walking on his left heel.
Methods: There was no KF ring.He was restless and fidgety.He had dysarthria related to laryngeal dystonia.There was no bradykinesia, cerebellar signs, spasticity or sensory deficit.Basic laboratory investigations were normal.Peripheral smear did not reveal acanthocytes.MRI brain, echocardiography, nerve conduction study and electroencephalography were normal.Copper studies were normal.Viral markers, ASO titre, anti DNAase B were normal.Routine CSF study, serum vasculitic profile, auto immune markers and anti cardiolipin antibody were normal.Genetic testing for ATP1A3 gene exon 21 mutation showed amino acid substitution of arginine for glycine at codon 960, suggestive of DYT12.He received levodopa, trihexyphenidyl, and tetrabenazine with no benefit.
Results: Our patient had certain atypical features: 1) seizure at onset, 2) right hemichorea, 3)lower limb involvement 4)No parkinsonism.ATP1A3 gene encodes the Na+K+ ATPase pump, which is widely distributed throughout the neurons, which may explain the varying phenotypes of the disease.
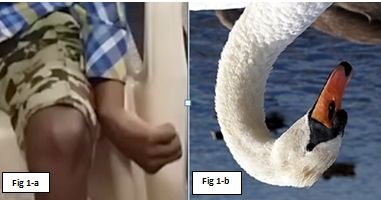

Conclusions: This patient had his left upper limb positioned like the neck of a swan (figure 1), and this has been seen in previously described case of ATP1A3 mutation associated rapid onset dystonia parkinsonism.This phenomenology “SWAN NECK” upper limb deformity seen in previously reported case may be a clinical clue to diagnosis. Presented in video challenge in MDSICON 2018, Bengaluru
References: 1. Dobyns, W. B. et al. Rapid-onset dystonia-parkinsonism. Neurology 43, 2596–2602 (1993). 2. de Gusmao, C. M., Dy, M. & Sharma, N. Beyond Dystonia-Parkinsonism: Chorea and Ataxia with ATP1A3 Mutations. Mov. Disord. Clin. Pract. 3, 402–404 (2016). 3. Brashear, A. et al. The phenotypic spectrum of rapid-onset dystonia-parkinsonism (RDP) and mutations in the ATP1A3 gene. Brain J. Neurol. 130, 828–835 (2007). 4. Sweney, M. T., Newcomb, T. M. & Swoboda, K. J. The Expanding Spectrum of Neurological Phenotypes in Children With ATP1A3 Mutations, Alternating Hemiplegia of Childhood, Rapid-onset Dystonia-Parkinsonism, CAPOS and Beyond. Pediatr. Neurol. 52, 56–64 (2015). 5. Termsarasab, P., Yang, A. C. & Frucht, S. J. Intermediate Phenotypes of ATP1A3 Mutations: Phenotype–Genotype Correlations. Tremor Hyperkinetic Mov. 5, (2015).
To cite this abstract in AMA style:
A. Elavarasi, V. Goyal, V. Vishnu, M. Singh, P. Srivastava MV. Rapid onset hemidystonia-hemichorea in DYT 12: Is “SWAN NECK” limb deformity a clinical sign? [abstract]. Mov Disord. 2018; 33 (suppl 2). https://www.mdsabstracts.org/abstract/rapid-onset-hemidystonia-hemichorea-in-dyt-12-is-swan-neck-limb-deformity-a-clinical-sign/. Accessed July 13, 2026.« Back to 2018 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/rapid-onset-hemidystonia-hemichorea-in-dyt-12-is-swan-neck-limb-deformity-a-clinical-sign/