Session Information
Date: Sunday, October 7, 2018
Session Title: Dystonia
Session Time: 1:45pm-3:15pm
Location: Hall 3FG
Objective: Determine reliability and feasibility of telemedicine evaluation of Cervical Dystonia (CD).
Background: Many CD patients receiving botulinum toxin (BoNT) injections are not able to follow up in clinic after treatment. Outcome is determined by patient recollection. Telemedicine allows patients to be evaluated with validated rating scales at home and provide real-time information regarding response to treatment and side effects.
Methods: Patients diagnosed with “spasmodic torticollis” and “cervical dystonia” who were ≥18 years old and scheduled for BoNT injection were recruited. Participants required a compatible computer or mobile device and access to high-speed internet. Patients were trained and examined using a standardized protocol. TWSTRS motor severity subscores were obtained by telemedicine and in person on consecutive days. Follow-up telemedicine visit was scheduled 4-6 weeks after injection. Agreement between the telemedicine and in-person TWSTRS scores was assessed using a weighted kappa statistic and intra-class correlation coefficient. Feasibility was determined by the number of enrolled subjects who completed all visits.
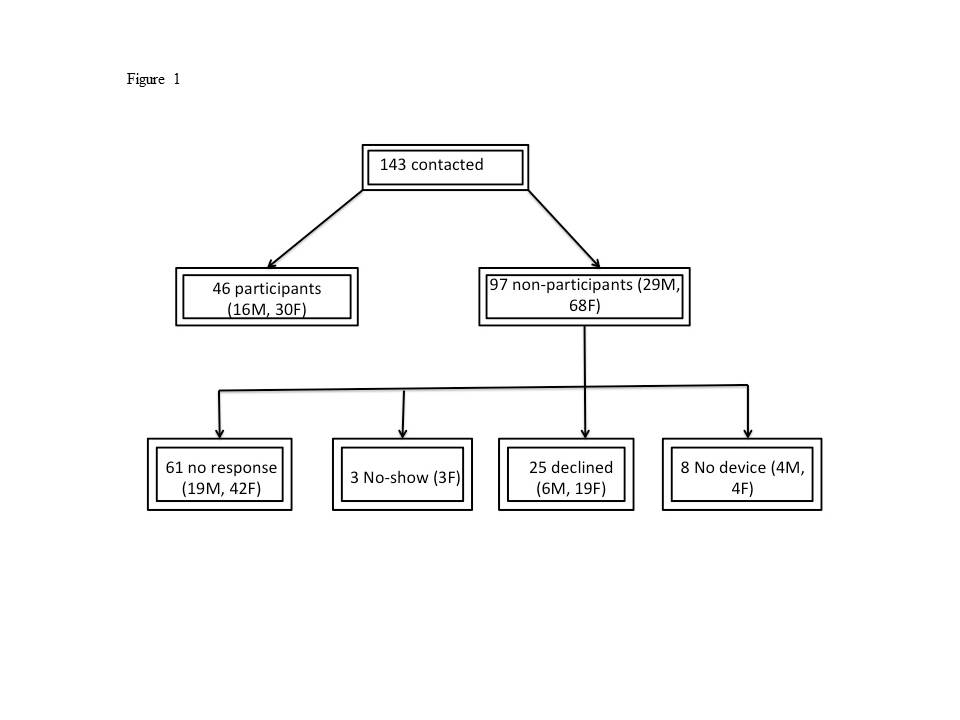
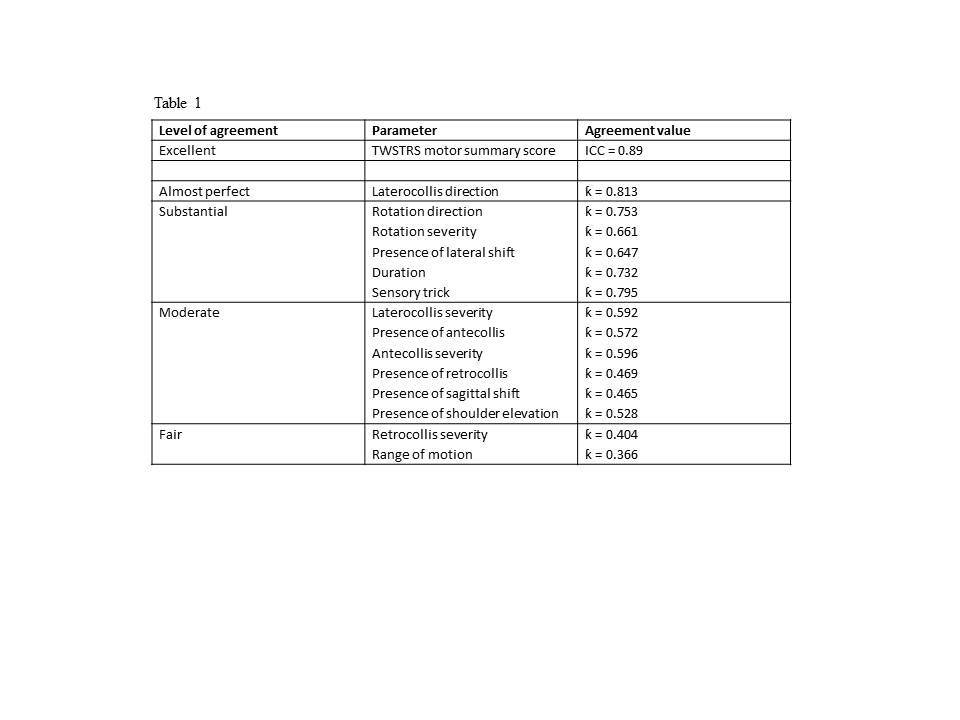
Results: 143 patients were recruited (98F/45M, mean age 59.48 ± 12.45) of which 46 were evaluated. Sixty-three percent of non-participants did not respond, 27% declined, 8.5% had no compatible device, and 3.2% missed their scheduled appointment (Figure 1). No participants had prior experience with telemedicine. TWSTRS motor severity summary score showed excellent intra-rater agreement (ICC = 0.89). Laterocollis direction (ƙ = 0.813) showed near perfect agreement. There was substantial agreement for rotation direction (ƙ = 0.753), rotation severity (ƙ = 0.661), presence of lateral shift (ƙ = 0.647), duration (ƙ = 0.732) and presence of sensory trick (ƙ = 0.795). There was moderate agreement for laterocollis severity (ƙ = 0.592), presence of antecollis (ƙ = 0.572), antecollis severity (ƙ = 0.596), presence of retrocollis (ƙ = 0.469), presence of sagittal shift (ƙ = 0.465) and presence of shoulder elevation (ƙ = 0.528.). Fair agreement was found for retrocollis severity (ƙ = 0.404) and range of motion (ƙ = 0.366) (Table 1). All participants were successfully trained and 96% of participants completed all three visits on time.
Conclusions: Telemedicine evaluation of CD provides similar ratings as live evaluation. Feasibility was demonstrated as 100% of participants completed successful telemedicine training and 96% completed all three visits on time.
References: 1. Werle RW, Takeda SY, Zonta MB, Guimaraes AT, Teive HA. The physical, social and emotional aspects are the most affected in the quality of life of the patients with cervical dystonia. Arq Neuropsiquiatr 2014;72:405-410. 2. Gill CE, Manus ND, Pelster MW, et al. Continuation of long-term care for cervical dystonia at an academic movement disorders clinic. Toxins (Basel) 2013;5:776-783.
To cite this abstract in AMA style:
A. Fraint, G. Pal, G. Stebbins, C. Comella. Reliability and Feasibility of Telemedicine Evaluation of Cervical Dystonia [abstract]. Mov Disord. 2018; 33 (suppl 2). https://www.mdsabstracts.org/abstract/reliability-and-feasibility-of-telemedicine-evaluation-of-cervical-dystonia/. Accessed July 5, 2026.« Back to 2018 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/reliability-and-feasibility-of-telemedicine-evaluation-of-cervical-dystonia/