Objective: To describe clinical and local field potential changes in an adolescent with tardive dystonia after bilateral globus pallidus interna (GPi) DBS.
Background: Tardive dystonia (TD) is a complication seen with chronic use of dopamine receptor-blocking agents (DRBAs). TD can be debilitating and refractory to medical management. GPi-DBS has been shown to be an effective treatment for TD, though literature on adolescents is limited.
Method: Review of medical and video records of an adolescent with medically refractory TD treated successfully with GPi-DBS.
Results: This patient is a 17-year-old male with autism, intellectual disability, Von Willebrand disease, and epilepsy who presented with 6 months of involuntary head and neck movements in the setting of 3 years of treatment with olanzapine and risperidone. The initial exam was notable for significant retrocollis. Whole genome sequencing revealed a heterozygous variant of unknown significance in DHX37, which is not known to cause dystonia. Based on history and exam, the highest suspicion was for TD. DRBAs were tapered. Tetrabenazine, dantrolene, clonazepam, baclofen, benztropine and trihexyphenidyl were prescribed with no benefit. He eventually lost independent ambulation due to forceful cervical and truncal retropulsion from generalized dystonia. Due to concerns for safety (falls and potential neck injury), bilateral GPi DBS were implanted. His Burke-Fahn-Marsden Dystonia Rating Movement Scale score decreased from baseline of 108.5 to 70 at 6 months post-stimulation. Although generalized dystonia remains present, he has regained independent ambulation. Medication doses have been reduced significantly at the 7-month visit. Prior to turning on DBS, his GPi local field potential showed a beta-frequency band peak around 25 Hz. At 7-month visit, this peak has significantly decreased in amplitude (Figure 1).
Conclusion: GPi-DBS can be an effective treatment for TD in adolescents and local field potential provides an opportunity to further understand the effects of pallidal stimulation.
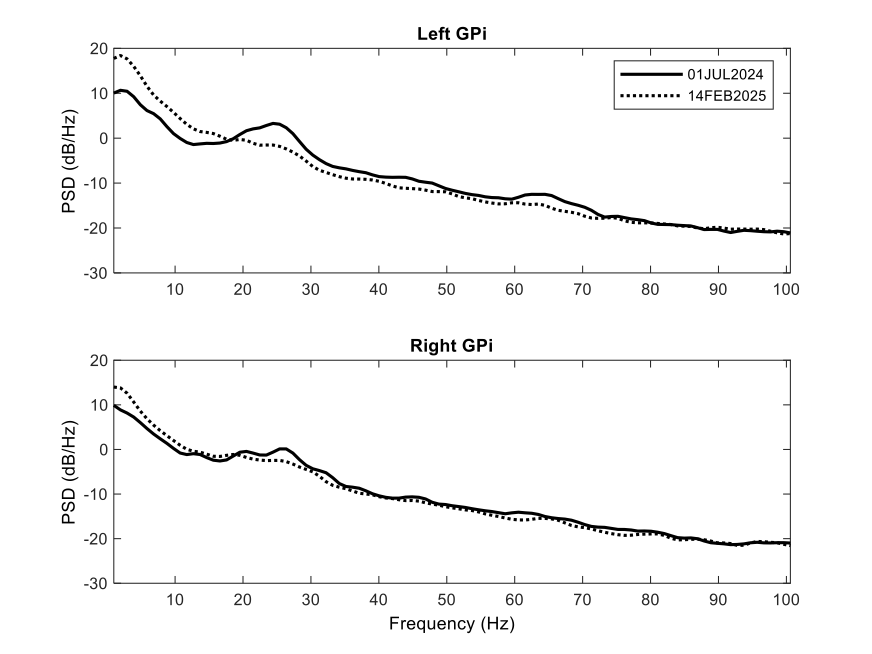
Figure 1
References: Badarny S, Nassar R, Badarny Y. Tardive Syndrome Is a Mysterious Phenomenon with Different Clinical Manifestations-Review. J Clin Med. 2023 Feb 14;12(4):1498. doi: 10.3390/jcm12041498. PMID: 36836033; PMCID: PMC9967615.
Krause P, Kroneberg D, Gruber D, Koch K, Schneider GH, Kühn AA. Long-term effects of pallidal deep brain stimulation in tardive dystonia: a follow-up of 5-14 years. J Neurol. 2022 Jul;269(7):3563-3568. doi: 10.1007/s00415-022-10965-8. Epub 2022 Jan 27. PMID: 35083518; PMCID: PMC9217904.
David Ledingham, Mark Baker, Nicola Pavese. Local field potentials: Therapeutic implications for DBS in dystonia including adaptive DBS for dystonia, Deep Brain Stimulation, Volume 5, 2024, Pages 4-19, ISSN 2949-6691, https://doi.org/10.1016/j.jdbs.2024.03.003.
To cite this abstract in AMA style:
HB. Burks, T. Larsh, J. Skoch, DL. Gilbert, SW. Wu. Restoration of Ambulation in an Adolescent with Tardive Dystonia after Pallidal DBS [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/restoration-of-ambulation-in-an-adolescent-with-tardive-dystonia-after-pallidal-dbs/. Accessed April 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/restoration-of-ambulation-in-an-adolescent-with-tardive-dystonia-after-pallidal-dbs/